Download
1 / 4
40 likes | 193 Views
KH. KH. KH. KH. Case 8. Patient KH (aged 1 year) referred for CF testing in October 2006: Possible diagnosis of CF 3 sweat tests – 1 positive result No mutations detected on the ELUCIGENE CF29 kit. Further analysis: Multiple exon DNA sequencing;

E N D
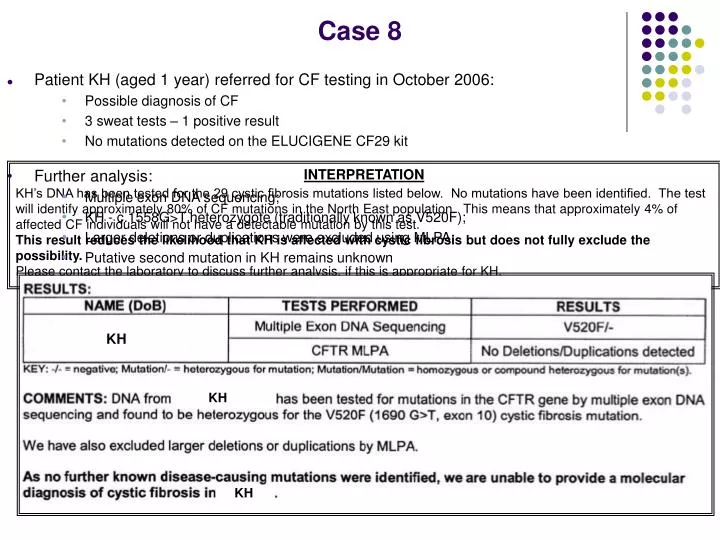
KH KH KH KH Case 8 • Patient KH (aged 1 year) referred for CF testing in October 2006: • Possible diagnosis of CF • 3 sweat tests – 1 positive result • No mutations detected on the ELUCIGENE CF29 kit • Further analysis: • Multiple exon DNA sequencing; • KH - c.1558G>T heterozygote (traditionally known as V520F); • Larger deletions or duplications were excluded using MLPA; • Putative second mutation in KH remains unknown INTERPRETATION KH’s DNA has been tested for the 29 cystic fibrosis mutations listed below. No mutations have been identified. The test will identify approximately 80% of CF mutations in the North East population. This means that approximately 4% of affected CF individuals will not have a detectable mutation by this test. This result reduces the likelihood that KH is affected with cystic fibrosis but does not fully exclude the possibility. Please contact the laboratory to discuss further analysis, if this is appropriate for KH.
polyT 17b CA/TA KM19 XV-2c J3:11 ~190Kb ~55Kb ~240Kb ~189Kb 1 2 7T 1 2 2 2 7T 1 2 2 1 7T 2 2 2 1 7T 3 2 1 2 7T 1 2 2 1 7T 3 2 Case 8 • Carrier testing: • Parents of KH (JH & CW) expecting second child (December 2008); • Referred for testing to: a. Establish carrier of the rare mutation; b. Identify a high risk allele for early postnatal testing • Linkage Analysis: • A series of microsatellite markers from the CFTR locus were typed in JH & CW; 1. XV-2c; 2. KM19; 3. CFTR intron 8 poly T; 4. J3.11 5. CFTR intron 17b CA/TA Position of the markers tested in relation to the CFTR gene Markers CV-2c KM19 Intron 8 polyT 17bCA/TA J3:11 - Intron 17b CA/TA marker partially informative
Case 8 • Summary: • CW - c.1558G>T mutation • High risk allele identified in JH • Prenatal testing now available (assuming a correct diagnosis of CF in KH) • No further referrals received by the laboratory to date INTERPRETATION CW and JH have been tested for the c.1558G>T mutation, known to be present in their daughter. No mutation has been identified in JH, but a single copy of the familial mutation was found in CW. A series of microsatellite markers from the CFTR locus have been typed in CW, JH and KH. The intron 17b CA/TA marker is partially informative in this family. Assuming a correct diagnosis of CF in KH, prenatal testing can be offered on the basis of direct detection of the c.1558G>T mutation and detecting segregation of the maternal high risk allele using the intron 17b CA/TA microsatellite. Carrier testing for the c.1558G>T mutation can also be offered to family members where appropriate.
Case 8 Discussion Points – MJS & DOR • Likelihood of an unidentified CFTR mutation after sequencing all 27 exons and intron-exon boundaries, plus MLPA • Reliability of linked markers in the absence of a CFTR mutation