Download

1 / 31
310 likes | 326 Views
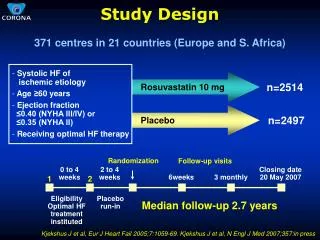
Prospects for stopping treatment : Should this be in a clinical trial? CML patient & carer meeting 2015 Hammersmith Hospital, 14 th November 2015 Richard Clark Royal Liverpool University Hospital. STIM Study Design. 100 patients.

E N D
Prospects for stopping treatment: Should this be in a clinical trial?CML patient & carer meeting 2015Hammersmith Hospital, 14th November 2015Richard ClarkRoyal Liverpool University Hospital
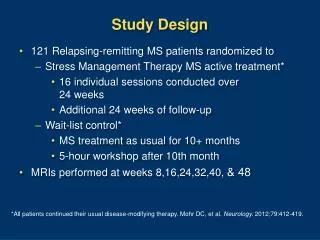
STIM Study Design 100 patients Q- RT-PCR from peripheral blood every month in the first year and every 2 months thereafter STOP Start Imatinib CMR Sustained deepMR for ≥ 2 years Five BCR–ABL analyses by RT-qPCR during these 2 years Sixth datapoint checked in centralized laboratory Mahon FX et al. The Lancet Oncology, 2010;11(11): 1029-1035.
100 CCR 1 BCR-ABL PCR % MMR 0.1 ~MR4 (level of detection) 0 12 15 18 21 24 30 36 42 Time (months)
STIM study results (Sept 2015) 100 patients 62 events (61 molecularrecurrences) At6 months: 43% ( 95%CI : 33 – 52) At24 months : 38% (95% CI: 32 – 51) Median follow up: 65 months (range 10-84) Mahon FX, Personal communication
Definition of molecular recurrenceacross discontinuation studies Rousselot P et al., Blood. 2007;109:58–60. Mahon FX, et al, Lancet Oncol. 2010; 11:1029-35. Ross D, et al. Blood. 2013;122:515-522. Takahashi N, et al. Haematologica. 2012;97:903-906.
Treatment free remission using loss of MMR to define molecular recurrence • 61% • Rousselot P et al., J Clin Oncol. 2014 Feb 10;32(5):424-30
Disease Burden and Molecular Response Number of Leukaemic Cells RUGBY BALL 1012 1011 1010 109 108 107 106 GrapeFruit Walnut Overallsurvival Grain of rice Stableresponse No risk of progression Less than grain of sand • Undetectable BCR-ABL mRNA transcript by real-time quantitative and/or nested PCR in 2 consecutive blood samples of adequate quality (sensitivity > 104)* Possibilityto discontinue therapy Baccarani M, et al. J ClinOncol. 2009;27(35):6041-6051 Radich JP. Blood. 2009;114:3376-3381
100 CCR 1 BCR-ABL PCR % MMR 0.1 ~MR4 (level of detection) 0 12 15 18 21 24 30 36 42 Time (months)
DESTINY De- Escalation and Stopping Treatment of Imatinib, Nilotinib or sprYcel in patients with excellent control of chronic myeloid leukaemia CI = Richard Clark, Liverpool
DESTINY Halve treatment: Imatinib 200mg Nilotinib 200mg 2xday Dasatinib 50mg Monitor monthly for 12 months If PCR remains below 0.1%, then stop. Further follow-up, monthly for a year then 2-monthly Associated lab tests that were not attempted in STIM
PCR alternate months in months 26-37 DESTINY PCR monthly until month 25 De-escalate TKI (13 months) Stop TKI 0 12 13 37 MONTHS
DESTINY recruitment: Target = 168 Sites: Royal Liverpool U Hospital 39 Hammersmith, London 22 Beatson, Glasgow 15 Kent and Canterbury 12 St James, Leeds 12 Nottingham City Hospital 10 King’s College Hospital, London 8 Hereford 7 Freeman Hospital, Newcastle 7 Heartlands, Birmingham 6 Royal Devon & Exeter 5 Salisbury 5 Colchester General 5 North Bristol (Southmead) 4 Queen Elizabeth Birmingham 4 UHW, Cardiff 4 Churchill, Oxford 3 Aberdeen Royal Infirmary 3 Manch’ster Royal Infirmary 2 Addenbrookes, Cambridge 1 TOTAL 174 Recruitment completed April 2015. 174 patients.
Questions from stopping studies Do patients feel better on de-escalation/stopping?? How many patients don’t go into stopping studies and why?? Can some patients who relapse on stopping manage well on lower doses?? Is very deep remission (MR 4.5)essential for stopping?? What is the minimum safe time of prior TKI before attempting stopping?? Are ‘hares’ more likely to stop successfully than ‘tortoises’? Can we predict successful stoppers by: more sensitive PCR? (Hammersmith) by immune profile? (Liverpool) by residual marrow leukaemia? (Glasgow)
Questions from stopping studies Do patients feel better on de-escalation/stopping?? How many patients don’t go into stopping studies and why?? Can some patients who relapse on stopping manage well on lower doses?? Is very deep remission (MR 4.5)essential for stopping?? What is the minimum safe time of prior TKI before attempting stopping?? Are ‘hares’ more likely to stop successfully than ‘tortoises’? Can we predict successful stoppers by: more sensitive PCR? (Hammersmith) by immune profile? (Liverpool) by residual marrow leukaemia? (Glasgow)
When are the results of DESTINY expected? Trial closed in April 2015. No-one has progressed, and no other serious problems. 100 patients will have completed de-escalation by December (next month) I will see results just before Xmas Analysis by end of February 2016: to be shared with scientific teams. De-escalation results on all patients to be made public in June 2016. Complete stopping results likely in June 2018.
What next? Prospects for stopping treatment: Should this be in a clinical trial? Ideally yes, to maximise our information/understanding Not possible at present. Need some data from DESTINY: It and EUROSKI will report in June 2016 (European Haematology Association)
What next? Need some data from DESTINY:
Estimations of the future prevalence of CML in the TKI era Based on: The annual mortality rate on TKI therapy compared with a age-matched, non-CML population The incidence of CML (4800 new cases per annum in the USA) The anticipated population growth The ageing of the population Huang et al, Cancer 2012; 118: 3123-7
Numbers of patients monitored at Royal Liverpool University Hospital ~ 30 new patients per annum ~ 1 death per annum (often due to ‘natural’ causes)
Improvement of Survival of CML by Therapy 1983 – 2011 n = 3615 Imatinib, 2002 – 2011 5-year survival 90% 8-year survival 88% IFN or SCT, 1997 – 2003 5-year survival 71% Survival probability IFN or SCT, 1995 – 2001 5-year survival 63% IFN, 1986 – 1994 5-year survival 53% Hydroxyurea, 1983 – 1994, 5 yr surv. 44% Busulphan, 1983 – 1994 5-year survival 38% Year after diagnosis German CML Study Group, 2011.
Improvement of Survival of CML by Therapy 1983 – 2011 Imatinib, 2002 – 2011 (CML IV) 5-year survival 90% 8-year survival 88% Age matched non-CML population (US data) 5-year survival 93% 8-year survival 87% Survival probability Year after diagnosis
174 CML patients & their 20 teams taking part in DESTINY Acknowledgements
100 CCR 1 BCR-ABL PCR % MMR 0.1 ~MR4 (level of detection) 0 12 15 18 21 24 30 36 42 Time (months)
STIM: estimates of CMR / MR4 after discontinuation of imatinib The overall probability of maintenance of CMR at 24 and 36 months was 39% (95% CI 29-48). Molecular recurrence occurred in 61 pts with 58 occurring during the first 7 months, and 3 late recurrences at month 19, 20 and 22, respectively
Can we cure CML? • “Absence of long-term leukaemia relapse after treatment discontinuation?” • Requires at least sustained deep MR in TKI treated patients • We may never be able to prove that cure requires the eradication of residual leukaemic cells
Conclusions The subset of patients with deep MR leading to cessation of treatment is heterogeneous. Around 40% of CML patients with stable deep MR on imatinib for at least 2 years are likely to remain in a prolonged TFR after treatment is stopped. The rate is around 60% if the loss of MMR is the criterion of molecular recurrence. A long-term follow-up of different cessation studies will be necessary to affirm cure.
Now that the DESTINY trial is closed to recruitment, what are the options for patients wishing to stop TKI? Need some data from DESTINY: Is de-escalation/stopping safe in MR4 but not MMR patients? Is monthly monitoring essential? If relapse rate on de-escalation is very high, then this needs to be gentler If relapse rate on de-escalation is very low, then could be more rapid/lower dose
EURO-SKI Study update: Final recruitment Patient recruitment (as of June 9, 2015)
Molecular relapse free survival EURO-SKI 200 interim patients – overtime, loss MMR=89 Relapseswithin 6 months, n=77 Molecular Relapse Free Survival At 6 months : 63 % (95% CI : 55% - 69%) At 12 months: 56 % (95% CI : 49 % - 63 %) At 18 months : 55 % (95% CI : 47 % - 61 %) Months from discontinuation of TKI Mahon et al. Blood (ASH 2014);124:abstract#151.
Questions • Can all patients be in sustained molecular relapse-free remission ? Is this a realistic goal? • Which molecular level is a realistic target to aim for before therapy is stopped? • What is the minimal duration of TKI pretreatment before stopping? • What is the minimal duration of MR4 before stopping? • Prognostic factors for TFR • What is the role of IFN pretreatment ?