Download

1 / 28
280 likes | 423 Views
Session 1 Background and Legislative Requirements. ClinicalTrials.gov Background. Dr. Deborah A. Zarin. ClinicalTrials.gov Team. Jerry Sheehan. Betsy Humphreys. Director Deborah Zarin Project Leads Annice Bergeris Nicholas Ide Alison Robbins Tony Tse Rebecca Williams

E N D
ClinicalTrials.gov Background Dr. Deborah A. Zarin
ClinicalTrials.gov Team Jerry Sheehan Betsy Humphreys Director • Deborah Zarin Project Leads • Annice Bergeris • Nicholas Ide • Alison Robbins • Tony Tse • Rebecca Williams Quality Assurance • John Frye • Cherryl Macalintal • Alex Valentine • Systems Development • Jane Fun • John Gillen • Alex Kostyukovsky • Russell Loane • Allison Yu • Domain Expert • William Harlan • Administration • Tamia Whitfield
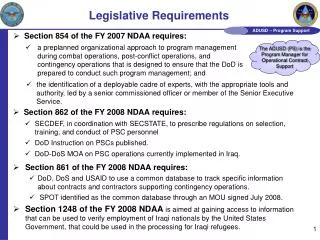
Ethical and Scientific Rationale for Increased Clinical Trial Transparency • Subjects put themselves at risk • Subject’s right to be informed • All available options, including ongoing trials • Previous research, including completed trials • Avoid redundant trials • Support Evidenced-Based Medicine (EBM) • Detect reporting problems • Lack of publication • Unexplained changes to protocol
The investigation was launched following concerns… • …although the ENHANCE trial ended in April 2006, the data had not yet been released. • …[the sponsors] did not register the clinical trial in a timely manner. • …[the sponsors] attempted to change the study endpoints, and thus the study results, prior to the public release of the results.
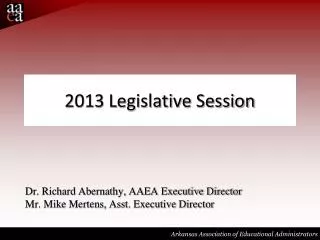
Source: Silverstein FE et al. JAMA. 2000 Sep 13;284(10):1247-55.
Kaplan-Meier estimates for ulcer complications according to traditional definition. Results are truncated after 12 months, no ulcer complications occurred after this period. Adapted from Lu 2001. Source: Jüni P, Rutjes AW, Dieppe PA. BMJ. 2002 Jun 1;324(7349):1287-8.
ClinicalTrials.gov • Prospective registry • Interventional and observational “trials” • Approved by IRB (or equivalent) • Conform to regulations of national health authorities • All sponsor types • All intervention types • Summary of key protocol items • Consistent with ICMJE and WHO • Links to publications, other info • Does not include unpublished results
Policies and Users Ottawa Statement Sponsor Policy (e.g., NIH, VA) PL 110-85 ICMJE Maine FDAMA 113 BPCA WHO ClinicalTrials.gov Recruitment (e.g., patients, physicians) Health Policy Makers Systematic Reviewers Journal Editors Research Funders
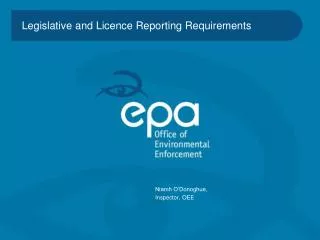
International Registries and Number of Trials (as of 2/4/08)
Characteristics of ClinicalTrials.gov Web-based registration system (PRS) Register through organizational accounts Key part of validation XML data upload (<20% records) Data are dynamic—”data provider” can modify data at any time Changes are tracked
ClinicalTrials.gov Statistics(as of 2/4/2008) Number Percent Total 50,564 100% Type of Trial* Observational 7,701 15% Interventional 42,836 85% • Drug & Biologic 32,835 • Surgical Procedure 10,856 • Behavioral, Gene Transfer, Other 4,809 • Device 2,628 International Sites US only 25,485 50% Non-US only 15,982 32% US & Non-US mixed 3,934 8% Missing 5,163 10% * 27 records missing Study Type information 21
ClinicalTrials.gov Statistics Cont.(as of 2/4/2008) NumberPercent • Trials by Data Provider • US Federal (including NIH) 16,430 33% • University, other 19,803 39% • Industry 14,331 28% • User Statistics • Page Views per month 20 Million • Unique visitors per month 500,000 22
Organizational Accounts Total 4,792 • Fed accounts 71 • NIH accounts 26 • Industry 1,783 • Other 2,912
Validation of Data for Registry • Issues • Quality Assurance: Are the entries as accurate and informative as possible? • Validation (w/o access to protocols): Is the fundamental information true? • QA Process at ClinicalTrials.gov • System of automated and manual checks • Staff works with data provider to correct/improve records • Links inserted
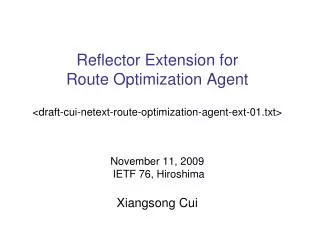
ENHANCE 2 1 3 Source: Kastelein JJ, Sager PT, de Groot E, Veltri E. Am Heart J. 2005 Feb;149(2):234-9.
Primary Outcome Measures: • Change in ultrasound-determined average carotid artery intima-media thickness (IMT) on a per subject basis between baseline and endpoint. [ Time Frame: 24 months ] • Primary Outcome Measures: • Change in ultrasound-determined average carotid artery intima-media thickness (IMT) on a per subject basis between baseline and endpoint. [ Time Frame: 24 months ]