Download
1 / 31
460 likes | 1.59k Views
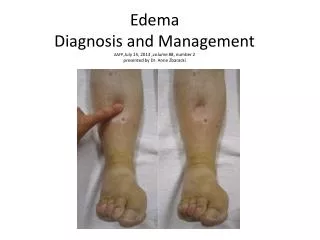
Introduction to Manual Edema Mobilization (MEM). -or- Why light touch is the right touch… -and- Why edema reduction matters. Sandy Sublett, PT, DPT, OCS, CLT. Special thanks to Sandra Artzberger MS, OTR, CHT, CLT. WHY’s for Reducing Edema. Edema is both visible and non visible

E N D
Introduction to Manual Edema Mobilization(MEM) -or- Why light touch is the right touch… -and- Why edema reduction matters
Sandy Sublett, PT, DPT, OCS, CLT Special thanks to Sandra Artzberger MS, OTR, CHT, CLT
WHY’s for Reducing Edema • Edema is both visible and non visible • Decrease edema, pain reduces because less pressure on neuroreceptors • Decrease in edema reverses path to fibrosis, stiff joints, ROM limitations. • Constituents leading to fibrosis are found in thick “slow to rebound edema” that only the lymphatic system can remove • Lymphatic system has specific methods to be activated, one is MEM
Venous System • A continuous system going from the heart to the extremities --arterial, then back to the heart --via venous system • Heart acts as a pump • Histologically on a capillary level, the arteriole and venule are connected
Lymphatic System • Lymphatic system begins at capillary level and ends in venous system: R&L Subclavian Veins • Lymph System provides its own pump • internal vacuum from pressure changes • external stimulation
5 Main Lymphatic Structures: when all activated, edema from a congested lymph system successfully reduces • Initial lymphatics (capillaries) and pre collectors (ABSORB)--located in dermis tissue • Collector lymphatics (Conduct)--deeper tissue • Lymph Nodes (Cleanse, Resist, Conduct) • Lymph Trunks (Conduct) • Thoracic Duct (Conducts)--anterior to and parallels spinal cord
Initial Lymphatic Anatomy • Lined with overlapping endothelial cells • Junctions between the endothelial cells open and close creating a pumping action • Connector filaments (microfibrils) extend from the lymphatic to connective tissue
Clinical Problem: lack of understanding of the role lymphatics play in edema reduction • Lymphatics are the only system able to carry away plasma proteins and other large molecules that become congested in the interstitium post tissue trauma. • Lymphatics are the “over flow” system. When the venous system reaches maximum capacity to remove fluid Lymphatics will remove the fluid if they aren’t collapsed by tight compression. Collapse=edema=decreased motion.
Congestion of protein rich fluid leads to fibrosis. Congestion of bacteria, tissue waste products, etc. that only the lymph system can remove decreases macrophage activity, decreases oxygen to tissue thus delaying wound healing • Many total joint patients have long standing (chronic, pre-op) edema issues. • Lymphatic absorption net is 1/8th inch below skin, one cell thick, more than 40mmHg collapses the net preventing absorption. • of soft tissue structures
Manual Edema Mobilization (MEM) definition • A method of edema reduction for a lymph system over - load (compromise) as seen with sub-acute and chronic upper and lower extremity edema post trauma, surgery, chronic venous insufficiency, and stroke. It is a multi-faceted Tx. method of lymphatic vessel stimulation to congested high protein edema.
MEM Definition Con’t: • MEM addresses post surgical and tissue trauma edema for over-whelmed (congested) intact normal nodes and lymphatics. • Not appropriate for primary or secondary lymphedema because extensive re-routing isn’t taught. • MEM Pump Point technique is appropriate to include with both sub-acute edema and lymphedema
Anatomical Rationale for Tx. “Keys” • Diaphragmatic breathing: creates a vacuum effect in the thoracic duct drawing lymph centrally from the periphery (Kubic) • Exercise after each segment massaged: moves lymph faster proximally because ex. stimulates increase in lymphangion pumping 10 to 30x normal rate (Guyton & Hall)
Light massage or bandaging: 60 mmHg. pressure begins to close the initial lymphatics, completely closed at 75 mmHg. (Miller-Seale) on a flat surface. Initial lymphatics are where absorption takes place from the interstitium • Use induration softening devices: these create neutral warmth. Lymph flows best between the temperatures of 71.6 F and 105.8 (Kurz)
Key characteristics of MEM • Key: Start Central at Trunk: diaphragmatic breathing, trunk ex., axillae, trunk anastomoses • Light massage: “half the weight of hand, sliding skin over muscle,””U” shaped strokes ending toward proximal set of nodes, begins central at trunk and works distal to end of extremity. • Incorporates other soft tissue mob. techniques i.e. MFR, elastic taping, jt. mob.
Utilizes a MEM Pump Point program • Where necessary, includes a bandaging program and other induration softening methods. • Key: patient follow - through on a daily self management program--create a simple program that can be incorporated into ADLs such as at daily shower time. • Key: exercise of muscles (A or P) in the segment just massaged and at end of TX. do distal to proximal exercises.
MEM Contraindications~don’t do if: • Currently in active state of: • CHF, COPD, severe kidney failure, liver disease or decreased function, malnutrition, infection-localized or systemic (flu, bad cold), cellulitis, blood clots, presently suffering from asthma or allergies.
Check with physician if patient presents with: • history of: CHF, COPD, potential for blood clots, pregnancy, history of cellulitis, advanced renal failure, active cancer
Types of Edema • Acute Edema--initially a low protein edema that decreases with a bulky compressive dressing, icing, elevation, light retrograde massage. • Sub-Acute edema--persistent edema, 30 plus second rebound from being pitted, congested high protein edema. Tx: MEM, elastic taping, LE minimal bandaging program, MFR, Jt. Mob., MEM home program.
Chronic edema: present 3+ months, areas of degrees of induration, decreasing ROM. TX: MEM, elastic taping, MFR,Jt. Mob., induration softening tech., more extensive LE bandaging, MEM home program. • Lymphedema--primary or secondary: Low out put failure of the lymph system due to a permanent damage of the lymphatic system. TX: MLD, bandaging, skin care, exercise, home program and usage of MEM Pump Points
Complex or combined edema: a low protein edema that has developed a high protein component because the lymphatic system has become overloaded while attempting to remove the low protein. • Other Edemas i.e. Raynaud’s disease, osteoarthritis, rheumatoid arthritis, drug related edema-MEM could be ineffective or contraindicated
Chronic LE edema=complex edema=lymphedema related to venous insufficiency +
MEM is Appropriate for What Types of Orthopedic Edema • Sub-acute post surgical/trauma high protein edema--yes MEM • Post surgical/trauma chronic high protein edema--yes MEM • “Persistent high protein edema is glue”
Minimalistic MEM LE Patient Home Program for sub-acute edema • Diaphragmatic breathing, trunk exercise, “glute” sets, inguinal node stimulation, knees to chest exercise, “sweep” knees to hip crease, stimulate popliteal nodes, toe curls, ankle pumps, heel slides, knees to chest, “glute” sets, diaphragmatic breathing.
Garments are not worn at night because when leg horizontal there is no venous insufficiency • Garments provide graded compression-greater distally-to help prevent reflux of fluid • If minimal edema refill problem or minimal venous insufficiency non-medical grade compression knee highs might be adequate.
Video on edema management • https://www.youtube.com/watch?feature=player_embedded&v=8skWJk6pqvY