Download
1 / 48
511 likes | 733 Views
Thoughts on oral/sublingual titration with triazolam. The prohibition of multiple dosing may have unintended undesirable consequences Two smaller doses (2 x 0.25 mg) separated in time are safer than one larger dose (1 x 0.5 mg) Multiple dosing can prolong effect duration

E N D
Thoughts on oral/sublingual titration with triazolam • The prohibition of multiple dosing may have unintended undesirable consequences • Two smaller doses (2 x 0.25 mg) separated in time are safer than one larger dose (1 x 0.5 mg) • Multiple dosing can prolong effect duration • Dose stacking can provide limited titration • Faster onset, reduced variables with sublingual triazolam enhance titration ability USP Workshop
Safeguards for oral sedation beyond anxiolysis • Continual monitoring of patient for consciousness • Continuous monitoring of pulse oximetry, heart rate • Continual monitoring of blood pressure • Use of reversal agent if patient drifts into unconsciousness and cannot be aroused AGD White Paper
Proposed Changes to ADA Documents on Sedation • ADA Policy Statement: The Use of Sedation and General Anesthesia by Dentists • Housekeeping • Guidelines for Teaching Pain Control and Sedation to Dentists and Dental Students • Major changes in definitions, teaching of moderate enteral sedation • Guidelines for the Use of Sedation and General Anesthesia by Dentists • Major changes in definitions, performance of moderate enteral sedation
Proposed ADA Teaching Guideline Changes • Allows multiple dosing of triazolam up to 0.5 mg total dose within definition of minimal sedation when full effect of previous dose known • Requires 16 hour course for minimal enteral sedation (may include inhalation sedation as well) • Allows multiple dosing of triazolam beyond 0.5 mg within definition of moderate sedation • Requires 60 hour course for moderate enteral sedation to include management of 10 patients with IV access with faculty/student ratio of 1/3
Proposed ADA Use Guideline Changes • Requires dentist to be able to rescue patient “whose level of sedation becomes deeper than initially intended” • Requires ACLS or “appropriate dental sedation /anesthesia emergency management course in addition to 60-hour course for oral moderate sedation • Requires time-oriented anesthesia record with vital signs recorded continually
Flumazenil (Romazicon) • 0.1 mg/mL • 5 mL vials
Flumazenil (2) • Specific benzodiazepine receptor antagonist • Causes rapid reversal of: • Unconsciousness • Sedation • Amnesia • Psychomotor dysfunction
Flumazenil (3) • Most patients respond to dose of 0.6 - 1.0 mg IV • Resedation most common after large doses of benzodiazepine and long procedures • Monitor for up to 2 hr after administration
Flumazenil (4) • Adverse effects • Nausea and vomiting, agitation • Seizures in patients with epilepsy • Drug interactions • Benzodiazepine withdrawal • CNS stimulation with tricyclic antidepressants
Questions regarding flumazenil reversal • Rate of emergency progression with oral triazolam • Relative efficacies and onset times of intravenous versus intramuscular, other routes • Safety of standard dosing versus titration
Flumazenil effects: influence of route of administration in dogs Heniff et al: Acad Emerg Med 4:1115-8, 1997.
Comparison of 3 Routes of Flumazenil Administration to Reverse Benzodiazepine-induced Desaturation in an Animal Model • 0.5 mg/kg midazolam IV to produce respiratory depression (SaO2 to ≈90%) in anesthetized dogs • 2 minutes later given “reversal treatment • No injection control • 0.01 mg/kg (0.12-0.17 mg) IV flumazenil • 0.2 mg SM flumazenil • 0.2 mg IL flumazenil • Blood drawn at various times for flumazenil measurements Unkel et al: Pediatr Dent 28:357-62, 2006
1 ? Unkel et al: Pediatr Dent 28:357-62, 2006
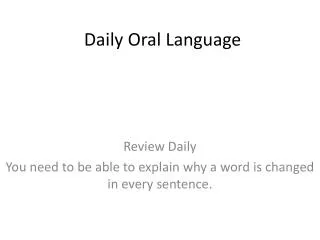
5 4 3 2 Tongue (n=5) IM (n=3) IV (n=2) 1 150 180 210 240 Observer Rating of Sedation Post Flumazenil (0.2 mg) Administration Sedation Score flumazenil admin. Time (minutes post-1st SL triazolam dose) Jackson et al: unpublished data
flumazenil admin. Jackson et al: unpublished data
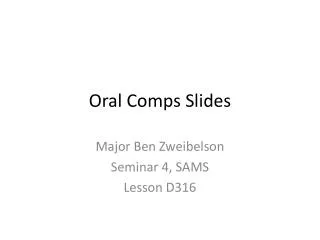
100 #569 80 #570 #571 #572 #573 #574 60 #575 #576 #577 #578 40 20 0 0 60 120 180 240 Psychomotor Function Assessment 10 Minutes Post-Flumazenil DSST Score Flumazenil Admin: Filled circles: IM Filled triangles: SL Open squares: IV flumazenil Time (minutes) (0.2 mg) Jackson et al: unpublished data
Rebound Sedation at the Time of Discharge Four subjects required an additional dose of flumazenil (0.2 mg, IV) 60 minutes after the initial dose (as determined by the anesthesiologist’s discharge criteria): • IV: 1 subject • IM: 1 subject • SL: 2 subjects Jackson et al: unpublished data
Lorazepam (Ativan) • Dosage forms: injection: 2 and 4 mg/mL in 1 and 10 mL vials and 1 mL Tubex; tablets: 0.5 , 1, and 2 mg • Directions: IV, 1-2 mg at start of case; oral, 2 (1-4) mg 1 hr before bedtime or 2 hr before treatment • Children: not recommended • Clinical duration: 6 hr • Recommendation: use for prolonged procedures or when treatment is delayed
Cardiac Disease and Dental Treatment • AHA/ACC Task Force on Perioperative Evaluation of Cardiac Patients Undergoing Noncardiac Surgery • Dental treatment and hypertension
AHA/ACC Task Force on Perioperative Evaluation of Cardiac Patients Undergoing Noncardiac Surgery
AHA/ACC Task Force on Perioperative Evaluation of Cardiac Patients Undergoing Noncardiac Surgery (2) We don’t treat these people
AHA/ACC Task Force on Perioperative Evaluation of Cardiac Patients Undergoing Noncardiac Surgery (3) Low risk We may have to consult physician re these patients
AHA/ACC Task Force on Perioperative Evaluation of Cardiac Patients Undergoing Noncardiac Surgery (4) Low risk We often don’t have to consult physician re these patients
Obesity and sedation • Two thirds of the adult population in the U.S. are obese or overweight • 17% of children ages 2 to 19 yrs are overweight • Prevalence has tripled in the past 2 decades • Obesity is a leading cause of restrictive lung disease
Body mass index [Weight (kg)] [Height (m)] BMI = 2 [89 kg] [1.89 m] Ex = = 24.9 2 >25 overweight; ≥30 obese; ≥40 morbidly obese
Overweight In children
Recognition of Potential Airway Difficulty • Mallampati-Samsoon classification • Thyromental distance • Joint mobility • Head and neck frontal and profile views • Tonsilar separation/obstruction
Mallampati-Samsoon classification of the airway • Class I - uvula, faucial pillars, soft palate • Class II - faucial pillars, soft palate • Class III - soft palate • Class IV - hard palate
Facial anomalies • Maxillary hypoplasia • Apert’s syndrome • Crouzon’s syndrome • Coronal craniosynostosis (Saethre-Chotzen syndrome) • Rubenstein-Taybi syndrome
Facial anomalies (2) • Mandibular hypoplasia • Treacher Collins syndrome • Hemifacial microsomia (Goldenhar’s syndrome) • Moebius syndrome (micrognathia 2O to neuromuscular deficit) • De Lange syndrome • Robin sequence
Sleep apnea • Obstructive sleep apnea is most common • Drugs with muscle relaxant properties can cause loss of airway • Drugs with respiratory depressant properties can cause loss of respiration • Sleep deprivation can increase chance for oversedation • Need for extended monitoring
Sleep apnea (2) • Repetitive episodes of upper airway obstruction during sleep • Accompanied by sleep disruption, hypoxemia, hypercarbia, cardiovascular stimulation • Often seen in obese or in patients with tonsillar hyhpertrophy or craniofacial abnormalities • Secondary cardiac and lung abnormalities Do you want to treat thesepatients?
Sleep apnea (3) • Most patients undiagnosed • Good questions to ask • Do you snore nightly? • Has anyone ever said that you stop breathing in your sleep? • Do you feel tired and groggy on awakening? • Do you fall asleep easily during the day? • Do you frequently have headaches in the morning? • Consider recommending sleep study for patients with positive findings