Download
1 / 41
410 likes | 506 Views
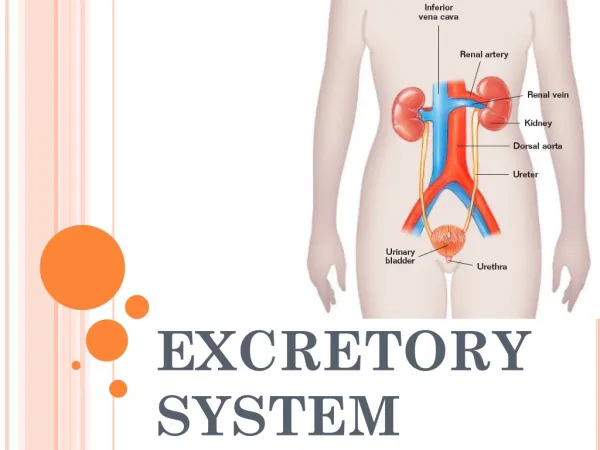
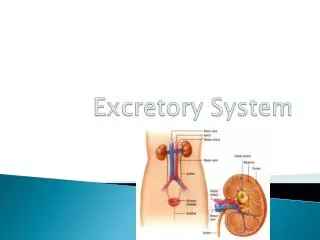
EXCRETORY SYSTEM. Function. Disposes of wastes & excess ions Regulates volume & chemical makeup of blood by maintaining proper balance between water & salts, acids & bases. UREA. Produces renin to regulate blood pressure & kidney function

E N D
Function • Disposes of wastes & excess ions • Regulates volume & chemical makeup of blood by maintaining proper balance between water & salts, acids & bases UREA
Produces renin to regulate blood pressure & kidney function • Produces erythropoietin to stimulate RBC production in bone marrow • Metabolizes vitamin D to its active form
Organs • Kidneys • Ureters • Urinary Bladder • Urethra
Anatomy of Kidney • Bean-shaped • Located between 12th thoracic vertebra and 3rd lumbar vertebra (partial protection) • Rt. kidney lies lower than left • Concave cleft on medial surface called- hilus which leads to the renalsinus
External anatomy • surrounded by renal capsule (protects from surrounding infection and trauma), • adipose capsule (holds kidneys in place and protects from trauma), • renal fascia (anchors).
Internal anatomy • renal cortex - outer region • renal medulla - inner region with cone shaped renal pyramids • renal columns separate pyramids • renal pelvis - continuous with the ureter leaving the hilus • major and minor calyces
Renal column Renal pyramid Renal calyx
Blood and Nerve Supply • renal arteries - deliver 1/4 total cardiac output to kidneys per minute • lobar arteries • interlobar arteries • arcuate arteries • Interlobular arteries
Nephron (this is where the action is!) • Interlobar, Interlobular, Arcuate, Lobar, Renal veins • Renal Plexus – sympathetic nerve fibers
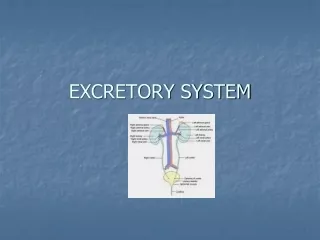
Nephron • over 1 million/ kidney; filtering unit of kidney; results in production of urine
renal corpuscle - consisting of glomerulus, Bowman's capsule • proximal convoluted tubule (PCT) • loop of Henle
distal convoluted tubule (DCT) • collecting tubule (urine collecting duct) • papillary ducts (collection of all collecting tubules)
Bowman’s Capsule • PCT • DCT • Loop of Henle • Collecting Tubule • Renal artery
7. Renal vein 8. Interlobular artery 9. Afferent artery 10. Glomerulus 11. Efferent artery 12. Peritubule capillaries
Kidney Physiology • 3 Steps involved in kidney filtration • Glomerular Filtration • Passive • Mechanical
based on hydrostatic pressure • enhanced by permeability of filtration membrane • filtration membrane consists of 3 layers
porous endothelium - prevents passage of cells & large proteins • thin basement membrane– charged to repel charged proteins
visceral membrane with slit-like openings; prevents passage of large plasma proteins • Net Filtration Pressure– Glomerular hydrostatic pressure + Bowman's hydrostatic pressure (opposing forces)
Filtration Rate: rate at which fluid is forced from blood into Bowman's capsule; dependent upon: - surface area - filtration membrane permeability - Net filtration pressure
Glomerular filtration rate • is proportional to Net filtration pressure • anything changing pressure at the membrane also changes the GFR, therefore higher blood pressure = higher GFR; dehydration = lower GFR
Tubular Reabsorption - reclamation of tubule contents • difference b/t filtrate & urine • filtrate - everything in blood plasma except proteins & cells • urine - wastes & unneeded substances
reclamation begins in PCT (both active/passive transport) • active - glucose; a.a., vit, Na, Ca, Cl, K, P,; most require a carrier molecule. When all carrier molecules are bound, excess are excreted into urine
passive - (diffusion, osmosis) • usually tied to active transport of Na • other anions move with Na to balance charges in the blood. • The anions that move depend on the blood pH • H2O moves passively (osmosis) due to its linkage to Na+
solvent drag occurs when filtrate becomes concentrated & solvent follows the concentration gradient back into the body • Explains why some drugs & toxins are not excreted easily
Nonreabsorbed substances • Urea (40% reabsorbed) • Creatine • uric acid • Tubule absorption capabilities • PCT most reabsorption occurs here Uric Acid
DCT • permeable to Na but not H2O • urine concentration determined here • dependent on blood pressure or volume • dependent on hormone release:
aldosterone - increases Na reabsorption & therefore H2O • ANF - opposes this • sex hormones • glucocorticoids
Tubular Secretion– Reabsorption in reverse • ammonia (secreted into the collecting tubule from the blood) • Active process • Some drugs (penicillin)
Pathology • Suppression- holding back • Pyuria- tract infection • Ptosis (hydronephrosis)- kinked ureter • Pyelonephritis– kidney inflammation
Pyelitis- inflammation of pelvis • Anuria- no output due to low pressure • Urethritis- inflammation of urethra • Cystitis- inflammation of bladder
Dysuria- painful urination • Incontinence- sphincter control • Retention- involuntary suppression • Diabetes insipidus– lack of ADH • Addison's Disease– not enough aldosterone • Excess Cl– indicate stone formation
Excess phosphates- alkaline urine • Cushing's Disease - hyperaldosteronism • Dehydration– low GFR • Hypotonic hydration–“water intoxication”; Hyponatremia, too much ADH • Renal calculi– kidney stones