Download
1 / 26
260 likes | 272 Views
This helpful assistant tool provides support in diagnosing and treating various conditions, including CHF, COPD, Afib, respiratory failure, acidosis, decubitus ulcer, malnutrition, and more. With its extensive knowledge and expertise, it helps healthcare professionals optimize patient outcomes.

E N D
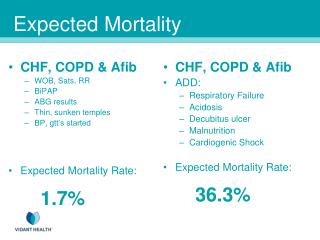
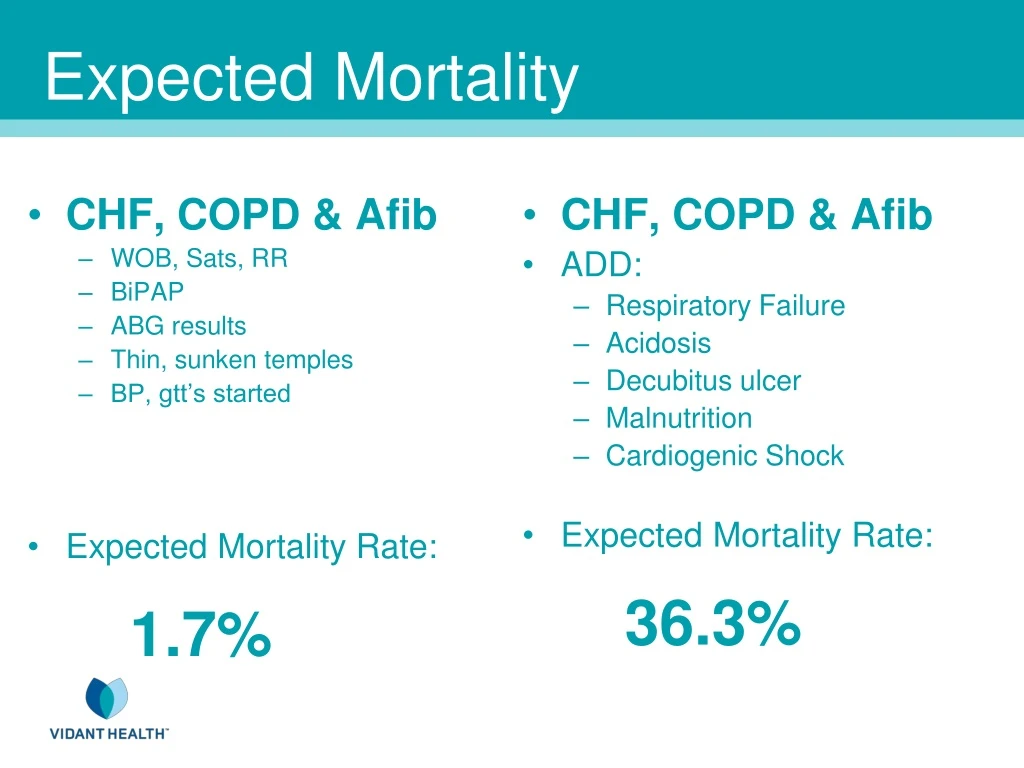
CHF, COPD & Afib WOB, Sats, RR BiPAP ABG results Thin, sunken temples BP, gtt’s started Expected Mortality Rate: 1.7% CHF, COPD & Afib ADD: Respiratory Failure Acidosis Decubitus ulcer Malnutrition Cardiogenic Shock Expected Mortality Rate:36.3% Expected Mortality
PNA Acute COPD Mortality Rate:0.3% Expected Mortality • PNA • Acute COPD • Add: • Malnutrition • Decubitis Ulcer • Mortality Rate:2.3% • PNA • Acute COPD • MODIFY: • Malnutrition, SEVERE • Decubitis Ulcer, STAGE IV • Mortality Rate: 9.2%
HCAPtranslates / codes to Simple pneumonia • Consider: PNA, possibly due to: • gram negative organism • Specific suspected organism
The Extra Step: • Include ALL chronic conditions • present and stable but managed
Cancer • Primary vs Secondary • Specify ALL metastatic sites • Active … Remission … Resolved • Include all associated diagnoses
Urosepsistranslates / codes to Simple UTI • Consider: Sepsis from a UTI
The Extra Step: • For each medication • Associated diagnosis • For each ordered study • Suspected diagnosis
When is a PE resolved?? • If PE is felt still present & being treated: • Identify as acute or subacute • Even if from a recent admission
ACUTE CHFtranslates / codes to CHF, not further specified • Consider: Specify diastolic &/or systolic Will then capture ACUTE
The Extra Step: • For each abnormal finding • (Lab, radiology, exam) • Describe clinical significance • INCLUDE suspected cause • NAME IT
ESRD • With fluid overload or pulmonary edema • Is it NON-CARDIOGENIC? • Or is it CHF • What is the cause (non-compliance?)
END STAGE COPD with continuous home O2 translates / codes to COPD only • Consider: • COPD, Acute Exacerbation • Acute & Chronic Respiratory Failure
The Extra Step: • Specify supportive facts for diagnosis • Quantify Risk Stratification
History of…?? • Is the condition truly resolved?Or is it chronic & stable with ongoing management
“Post-operative” Frequently translates / codes to complication • Caution on intended meaning: • TemporalvsCausativerelationship • Clarify if INTEGRAL to procedureor EXPECTED part of recovery period
The Extra Step: • Include ALL diagnosis being considered, worked up or treated • “possible”, “probable”, “likely” • Update diagnosis status • Ruled in or out • Remains possible
Altered Mental Status: Is it? • Acute Confusion • Chronic dementia…or acutely worse? • Acute delirium • Encephalopathy • Include specific suspected causes
Symptoms (dyspnea, chest pain, dizziness, weakness, fever) translates / codes to ???? • Explicitly state suspected cause • d/t arrythmia, COPD, CHF, PNA, etc. • d/t unstable angina or CAD, pleurisy, GERD, chest wall pain • d/t hypotension / dehydration • likely source, or bacterial infection unknown source
The Extra Step: • Relate conditions & State connections • UTI due to Foley • specific conditions due to prior CVA • Manifestations & Sequela
Manifestations of disease WITHOUTExplicit linkage translates / codes to Uncomplicated DM, HTN • Consider – use adjective or “due to” • Diabetic nephropathy or Hypertensive CHF
The Extra Step: • Carry diagnoses throughout stay • Include ALL diagnoses at discharge • Acute • Chronic • Resolved during stay
Condition with “VS” (differential diagnoses) translates / codes to Condition ONLY • Consider: • Identify primary suspected cause (then follow with alternatives) • Clearly indicate RULED IN & OUT diagnoses
Use STRONG terms: • Failure • Shock • Coma • Encephalopathy
The Extra Step: • Renal Status • CKD Stage? • Acute Renal Failure due to …
Use STRONG Qualification & Links: • Acute, Acute on Chronic • Sub-acute, Chronic • Congenital • Exacerbated • Uncontrolled • Mild, Moderate, Severe • Due to, Secondary to • Unstable
The Extra Step: • Abbreviations • Always spell it out the first & last time • Different areas expertise & knowledge • Prevent confusion & errors