Download
1 / 31
310 likes | 510 Views
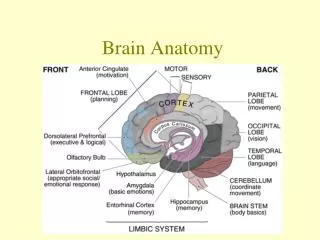
Skull & Brain. Imaging Techniques Plain……..M.M. before MRI for intra- occular metalic FB CT & MRI …standard investig . US Angiography….Limited to stenosis. aneurysm & AVM. Imaging Techniques. Plain ….

E N D
Skull & Brain Imaging Techniques Plain……..M.M. before MRI for intra-occularmetalic FB CT & MRI …standard investig. US Angiography….Limited to stenosis. aneurysm & AVM
Imaging Techniques • Plain …. Normal….inner & outer tables (compact) Diploic space ( spongy bone ) Sutures remain visible even after fusion. Metopic suture. Inconstant
Lytic & sclerotic lesions in the skull Lytic lesions • Metast. & M.M. • Geographic skull in histiocytosis X. Sclrotic lesions • Localized sclerosis… metastases
CT Brain • Normal CT • Abnormal CT cardinal signs -abnormal tissue density high density…recent hge, calcified and contrast enhancement low density….neoplasm, infarct, oedema
Abnormal CT…cont. • Mass effect ..compressed or displaced lateral ventricles Midline shift • Dilatation of ventricular system -CT with contrast; CT angio
MRI of brain • Multiplanar capability….extent of tumor. esp. for post. Fossa & craniovertebral junction. Disadvantage; inability to show calcification and bone details long scan time difficulty in monitoring critical patients
MRI Brain • Contrast Gadolinium MRA severe stenosis & aneurysm MRV venous sinuses
MRI Brain • It is more often possible to make a specific diagnosis with MRI than CT. • Demyelinating plaques of MS • AVM
Neurosonography • Hydrocephalus • Hemorrhage • Congenital abnormalities.
Brain Tumors • Glioma Solitary irregular mass surrounded by edema may compress or displace ventricle. usually hypodense may be hyper or mixed. may calcify most show partial enhancement. may be ring enhancement. Low in T1 , high in T2
Metastases may be of high or low density. surrounded by edema typically multiple a solitary metast. could not be diff. from a primary neither by CT nor by MRI
Meningioma arise from meninges of the vault, falx & tentorium. commonest sites are parasagittal region over the cerebral convexities & sphenoid ridge. Slightly hyperdense on native CT marked enhancement Acoustic neuroma; in the CPA near IAM.
Pit. Tumors: microadenoma < 10mm macroadenoma.> 10mm MRI
Cerebral infarction & hemorrhage Clinically similar CT is the initial exam. Hge….high density surrounded by edema. May be SAH or intraventricular. In Infarction ….CT normal initially. MRI diffusion Weighted Images.
SAH usually due to rupture aneurysm. CT is the best initial exam. The large aneurysms are seen by CT. MRA can show smaller aneurysms. Arteriography is the best. AVM may present with Hge….CT can show the AVM esp. with contrast. But MRI is better even without contrast.
Abscess Low density with ring enhancement
Head Injury: Fractures # more translucent # may branch abruptly Suture in known anatomical positions. Depressed #....dense. EDH can result from # through MMA groove.
CT in head injury CT should be done when there is: -deterioration in the conscious level. -worsening of neurological deficits. Extracerebral lesions -EDH.. biconvex. Associated with # High density for 2Wks. After 3-4Wks…..hypodense Isodense in between. -SDH…….concavoconvex
Fractures of the base & vault are easily seen in bone window Intracerbral lesions: -Edema- homogenous low density. -Contusions- patchy low density areas -Intracerebral hematoma Severe head injury can exist with no abnormal CT
Subarachnoid hemorrhage(hyperdensity in Sylvain fissures and interhemispheric fissures in CT scan)
Subdural hematoma(crescentic collection over the convexity of the hemisphere)