Download
1 / 29
310 likes | 506 Views
Functional genomic approach to ion channels as targets in complex polygenic disease J. Jay Gargus, MD, PhD Division of Human Genetics, Department of Pediatrics, and Department of Physiology & Biophysics University of California, Irvine. Complex Genetic Diseases.

E N D
Functional genomic approach to ion channels as targets in complex polygenic diseaseJ. Jay Gargus, MD, PhDDivision of Human Genetics, Department of Pediatrics, and Department of Physiology & BiophysicsUniversity of California, Irvine
Complex Genetic Diseases • Complex genetic diseases afflict at least 50 million individuals in the USA • Hypertension / Diabetes / Cancer • Manic-depression / Schizophrenia / Autism • High heritability, polygenic, +environment • genesmany genesnot only genes • Approach either based on • map position….weak, broad linkage signals • “random” association…LD.. high density SNPs • association w/functional candidate • how can function be defined??? • EVENTUALLY you MUST know the function anyway!
Major limitations of position-based search • map position….weak, broad linkage signals • Change diagnosis of 1 person can shift point of maximal lod several cM (megabases) • Dx is not clear, and phenotypes evolve • minimal ability to exclude weak effect gene from area • by definition ALL genes in complex disease are weak • “there will never be sufficient family material” • > 2000 families needed….Risch • very low power because of allele sharing with controls • few? none ? found yet ?caspase +DM • “random” association…LD.. high density SNPs • need ? > 500,000 sites genotyped in many people • need ? Haplotypes ? Current controversy • need faith in “common disease-common variant”
?Expect common alleles?could you “find” PKU in MR • MR has “locus heterogeneity” • many genes involved, often polygenic • untreated ...2% of MR caused by PKU • PAH major effect locus…simple AR inheritance • Frequent PAH disease alleles…q=.01 • polymorphic frequency; major effect single gene • 412 different alleles, “allelic heterogeneity” • Large gene, 90 kb, all exons w/ mutations • NO COMMON ALLELE • MOST simple Mendelian diseases have no common allele !!…..NO shared SNP
Problems finding best “candidate genes” • No function known • 1/2-1/3 of genes have no know function • No homolog in database • >1/3 of genes have no recognized homolog • No annotation in model systems • if a homolog is recognized, no phenotype identified • Such candidates must be “positional” only • implicated only by being co-localized with disease gene • proven by showing mutation, segregation, de novo hit • many genes in region; which association test to do first • Solutions: attempt to define functions • HOW…arrays etc.showing co-regulation, -evolution
Candidate gene association requires large scale sequencing • need to identify cSNPs in large number of candidate genes…coding / ?functional • ~1 per kb gene sequence; >60,000 known • 100 genes may have to be examined per disease • will need to examine large number of chromosomes from patients and controls • > 100 probands for given disease • (100 genes x 1.5 kb x 100 pts) = 15 Mb to examine • advantage to choosing “right” candidate early • advantage to multiplexing related diseases • “disease family” based on related pathophysiology
Problem defining how novel disease gene is pathogenic • Needed to identify potential target site for pharmaceutical intervention • Structural studies to suggest function • In vitro and In vivo Animal KO / TG models • Or..focused search of candidate gene family • signature, sequence or motif, lead to identification • known function (at least very broadly) • share common assays • it IS looking under the street light • in the wealth of targets that now exist, leave some behind & be willing to find ONLY those you will do something with immediately!
Focused Search ofGene Family Candidates • recognizable signatures to identification • share common functional assays • needed to assign specific function and screen drugs • general functions known • advantage to multiplexing related diseases • each multigenic and share some pathophysiology • potentially share some gene targets • mutual controls / misassigned candidate may hit • “candidate disease” within the “disease family”
Useful gene families • Many groups targeting • Receptors (5% of genes) • >75% of current drugs target these • most compounds in pharma libraries designed to these • Transcription factors (6% of genes) • largest family • Kinases (2.8% of genes) • G proteins (<1% of genes) • Relatively neglected • Ion channels (1.3% of genes)
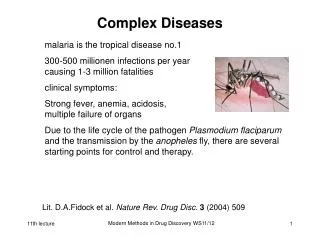
Ion channels produce DIVERSE Mendelian disease phenotypes • Heart ---arrhythmia • CNS --- seizures, ataxia, migraine • ? Neuropsychiatric diseases • Sk Muscle ---paralysis , paramyotonia • Vascular Sm Muscle---hypertension • Renal --- hypertension, electrolyte abn • Lung--- cystic fibrosis • Endocrine -- diabetes
Voltage-gated channels Potassium monomer Functional tetramer Na & Ca pseudo-tetramer
Commercial advantages to ion channel-based drug discovery • novel large class of targets • already proven & profitable targets • diabetes, arrhythmia, hypertension, baldness • implicated in major market diseases • serendipitous vs directed drug discovery • tissue-specific expression • offer approach to diverse clinical diseases • specificity minimizes side-effects
Practical advantages to ion channel-based drug discovery • “universal” High Throughput Screen assay • membrane potential and voltage sensing dyes • natural toxins • serve as standards for HTS • nM to pM affinity common • predictive atomic structures • focused combichem libraries can be synthesized • single-molecule sensitivity
Genome Database to Candidate Gene • Screen GDB /express cDNA • recognized by primary sequence motifs • channels readily expressed in vitro • can be studied for function as single molecules • Expression characteristics / uncompiled database of physiology and function • novel motifs • tissue distribution • functional channel features • binding affinity ligands / toxins • natures most potent toxins target channels • implicated pathophysiological mechanisms
cont..Genome Database to Candidate Gene • Map chromosomal position • Identify “candidate diseases” • chromosomal map position • implicated pathophysiological mechanisms • paralog disease genes • Test genetic hypothesis • SNPs / mutations • association / linkage
Ion Channel Target to Drug Discovery • Channel expression • Identification of toxin blocker • Definition of toxin structure • Definition of channel / toxin binding site • Definition of channel structure • Information-based library selection for designed High Throughput Screen • HTS hits optimized with functional assay
Illustration of annotation: KCNN3 and schizophrenia • gene motifs • neuronal calcium activated K channel • P region, six TM helices • polymorphic CAG repeat cassettes • late-onset neurodegeneration disease family • dominant disease • + or - “gain of function” mechanism • physiology • KCa control neuronal • excitability • Ca entry • secretion • apoptosis (via Ca load)
KCNN3 structure and putative function Exons 1 2 3 4 5 6 7 8 Poly-CAG After spike sHAP: S1 S2 S3 S4 S5 S6 NLS Met - Q14-29 COO Poly-gln 6P Q12 + NH3
KCNN3 and schizophrenia 2 • pharmacology • dopamine blockers treat the schizophrenia • correlation with affinity at D2 receptor • NMDA blockers produce the schizophrenia • PCP, MK801; KO mice lethal, hypomorph has “schiz” • phenothiazines treat schizophrenia • compete for binding w/ apamin, KCNN3 channel blocker • neuroanatomy / neurobiology • expressed in midbrain D2 dopaminergic pathways • D2 in nigrostriatal and mesolimbic (vta) • major controller of: • dopaminergic neuron pacemaker • bursting, chains of action potentials • dopamine secretion / monoamine secretion (5-HT, NE)
20mV 0.25ms Small-conductance Calcium-activated Potassium channel 3 (SK3) K+ Dopamine Dopaminergic Neuron
KCNN3 and schizophrenia 3 • association studies • long alleles over-represented in schizophrenia • found in many studies; not found in many • long alleles in ataxia and anorexia nervosa • novel alleles found in rare schizophrenia • truncation….clear channel phenotype • map positions • 1q21 by FISH and linkage..novel position for schiz • at site of Lod 6.5 linkage to schizophrenia--Canada • replicated in Icelandic and British cohort • neighborhood of Finland LD cohort • at site of Finland Asperger S. linkage • at site of Familial Hemiplegic Migraine 2 • functional studies of “pathogenic” alleles • in vitro and transgenic
Linkage analysis of 22 Canadian families segregating schizophrenia SKCa3 gene Brzustowicz et, al. (Science 2000)
4-bp deletion in a schizophrenic patient Exons 1 2 3 4 5 6 7 8 Poly-CAG S1 S2 S3 S4 S5 S6 Met NLS Met Q14-29 Poly-gln - Q14-29 6P COO Poly-gln 6P Q12 + Q12 NH3 + NH3
truncation of KCNN3 gene cause dominant negative effect on SKCa currents Exons 1a 2 3 4 5 6 7 8 SKCa3 Dopamine K+ Exons 1a 2 3 4 5 6 7 8 Truncated SKCa3 Dopamine K+
Acknowledgements Hiro Tomita George Chandy Guifeng Sun Michael Cahalan Kavita Bhalla George Gutman Emmanuel Fantino Vikram Shakkottai William Bunney Mark Miller Heike Wulff William Byerley Leslie Thompson Bob Moyzis Heiko Rauer Leena Peltonen…UCLA Aarno Palotie……UCLA