Download
1 / 39
400 likes | 709 Views
Dr. S. Parthasarathy MD., DA., DNB, MD ( Acu ), Dip. Diab . DCA, Dip. Software statistics Ph D physiology. Mahatma gandhi medical college and research institute, puducherry , India. C left lip and palate . Incidence . one child in every 700 is born with a cleft.

E N D
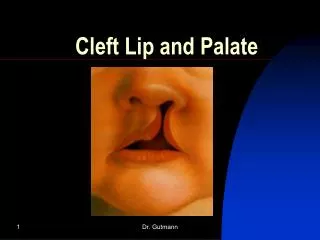
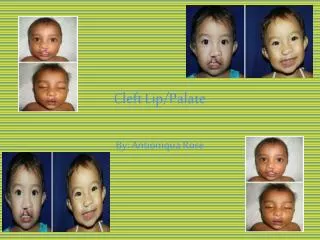
Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics Ph D physiology. Mahatma gandhi medical college and research institute, puducherry, India Cleft lip and palate
Incidence • one child in every 700 is born with a cleft. • For India, this translates into over 35,000 babies born each year with this condition
Variations • CLP is more common in males • cleft lips are usually left-sided. • Unilateral cleft lip 25% • Unilateral cleft lip and palate 25% • Bilateral cleft lip and palate 10% • Cleft palate alone 40%
Causes • “multi-factorial” • genetic predisposition • environmental issues such as drug and alcohol use, smoking, • maternal illness, infections • and lack of vitamin B folic acid
Why it happens ?? • clefts arise because of failure of fusion or • breakdown of fusion between the nasal and maxillary processes and the palatine shelves that form these structures at around 8 weeks of life.
CL may be reliably diagnosed at the 18-20 week scan. • CP is harder to see and can only be excluded on examination after delivery.
In 1912 – a surgeon wrote • the difference to the surgeon, between doing a cleft palate operation with a thoroughly experienced anaesthetist and an inexperienced one, is the difference between pleasure and pain!
Cleft lip cosmetic – tube fixing • Turnbul connection – invention of Bains
Preanaesthetic check up • standard preoperative history and examination • Special : • Associated congenital abnormalities • Pierre robin • Treacher collins • Goldenhar Syndrome
Preanaesthetic check up Treachercollins Pierre robin
Anaesthesia • Surgery is usually performed at 3 months for cleft lip repair 6 months for cleft palate • It may be delayed by the investigation of other problems or on-going airway difficulties – discussion
Waiting until 3 months of age gives time to detect most congenital abnormalities, and allows anatomical and physiological maturation.
Rule of 10- for cleft lip repair • 10 weeks of age • 10 gm% of Hb • TC < 10000 • 10 pounds weight
Preanaesthetic check up • Congenital heart diseaseoccurs in 5 - 10% of these patients • Chronic rhinorhoea. • This is common in children presenting for cleft palate closure and is due to reflux into the nose during feeds
Preanaesthetic check up • a history of snoring or obvious airway obstruction during sleep. • Anticipated difficult intubation. • Right ventricular hypertrophy and corpulmonale may result from recurrent hypoxia due to airway obstruction
Upper respiratory tract infections are particularly common at this age and carry an increased risk of airway complications and impaired wound healing • Appropriate antibiotics • Explanation to mother • nutrition
If not repaired • Feeding • Speech • Secretoryotitis media • Cosmetic
Premed • Sedative premedication – NO • the risk of airway obstruction • Atropine if necessary • Antibiotics • Oral paracetamol – 20 mg/kg
Induction • Inh. Halo or sevo • Iv access • Agent/ suxa / NDPs for intubation • No relaxants if mask ventilation is inadequate • Mask easy but tube difficult?
Difficult laryngoscopy • Difficult laryngoscopy (Cormack and Lehane views grade III or IV) occurs in up to 10% of ASA I patients for CLP repair. • Large alveolar defects may hamper laryngoscopy, a tendency for the laryngoscope to fall into the cleft; Packing with gauze, use of a straight blade may prevent this
Equipment • RAE tube • Armoured tube • Well fixed • JRMATP • ETCO2 monitoring must to detect accidental extubation
Other options • LMA has been successfully used to allow CLP repair in a child in whom intubation had proved impossible • more bulky, less secure than an endotracheal tube and its routine use is not advised. • Armoured LMA • Fibreoptic intubation - skilled personnel
Anaesthesia - tricks • oral pack to absorb blood and secretions. • A head ring and a roll under the shoulders is frequently used • local anaesthetic and adrenaline into the surgical field to reduce blood loss and improve the surgical field. It also provides some intraoperative analgesia
Controlled Vs spont • Spont • Ok if extubates • But small infants ?? • Controlled better
Periop pain relief • Morphine sulphate 0.1-0.2mg/kg intravenously is commonly used and provides good early postoperative analgesia. Fentanyl – choice • The use of opioids results in a smoother emergence and less crying on extubation. This reduces trauma to the airway and decreases the risk of postoperative bleeding.
Concerns • IV fluids • Blood for cleft palate repair • Temperature, NMJ • Postop analgesia • Suctioning cautious • No airway • Tongue stitch
Regional anaesthesia • Infra orbital block • The infraorbital nerve • supplies sensory • innervation to the • lower eyelid, • the side of the nose, • and the upper lip
Extraoral approach • intraoral approach • Don’t pierce the foramen • Give 2-3 ml of LA
Post op airway obstruction • Gag induced edema • postoperative airway obstruction include • subglottic edema, • flap edema, • increased oral secretion, • posterior displacement of the tongue, and an overlooked throat pack
In the postoperative period, arm restraints, which prevent elbow flexion, are routinely used to keep the child's hands away from the child's face. • Later naso tracheal tube?? , tonsillectomy???
Summary • 35,000 births in india every year?? • 3 months & 6 months(speech, feeds, otitis.cometic) • Look for other anomalies and airway • Premed – para • Induction sevo/ thio--- intubate/ LMA • Fixing, positioning ETT • No suction, airway , smooth ext. • Regional for analgesia