Download

1 / 53
530 likes | 816 Views
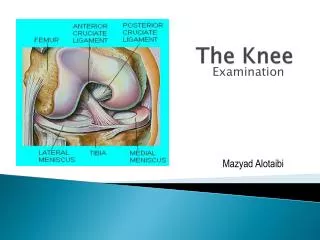
The Knee Complex . The Knee Complex. General Structure & Function Structure & Function of Specific Joints Muscular Considerations. General Structure. Joints of the Knee Complex. General Function. Provides very mobile link in an otherwise stable lower extremity

E N D
The Knee Complex • General Structure & Function • Structure & Function of Specific Joints • Muscular Considerations
General Function • Provides very mobile link in an otherwise stable lower extremity • Transmits loads from tibia/fibula to femur
Transverse plane • Medial and lateral • rotation • Sagittal plane • Flexion, extension
Knee Complex Movements • Frontal plane • Varus, valgus • Anteroposterior translation • Mediolateral translation
The Knee Complex • General Structure & Function • Structure & Function of Specific Joints • Muscular Considerations
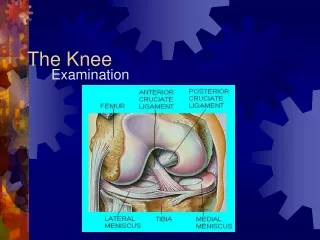
Structure & Function of Specific Joints • Tibiofibular Joint • Patellofemoral Joint • Tibiofemoral Joint
Tibiofibular Joint: Bony Structure Amphiarthrodial membranous syndesmosis joint
Structure & Function of Specific Joints • Tibiofibular Joint • Patellofemoral Joint • Tibiofemoral Joint
Purpose of Patella • Increase leverage of QF • Protect joint during knee flexion • ↓ pressure and distribute forces on femur • Prevent Fcompression on PT in resisted knee flexion • Disadvantage: ANT shear of QF
Patella Structure • Medial facet • Lateral facet • Odd facet (30%) M L
Largest sesamoid bone Least congruent joint Articular cartilage Vertical ridge Facets M L PF Articular Surfaces
Largest sesamoid bone Least congruent joint Articular cartilage Vertical ridge Facets Angle of femoral sulcus PF Articular Surfaces
INF & SUP Sliding Patellar tilt 11 MT as KN FL Med Lat Patellar Motion
Lateral rotation ACC MR of femur 6 through KN FL Medial rotation ACC LR of femur Patellar Motion
Patellalectomy • ↓ MA of QF (↓ strength 49%) • Q tendon friction • compressive stress on groove by Q tendon • Most evident in closed chain EXT • ECC QF in CC • Coupled w/ & assisted by hip & ankle movement • QF not needed in erect posture of CC
Extension Little effect overall
Slight Flexion Noticeable weakness
Extreme Flexion Noticeable weakness
0-60 • Contact area • MA of QF; 60 • ANT shear of QF 0-60 • Facet contact at 20
60-140 • contact area • MA of QF • No leverage in full FL
Overall • Medial facet most contact • Odd facet least contact
During Full Extension Full EXT • MA of QF • QF length • Patella very unstable
PF JRF • Amount of knee FL • Strength of QF contraction
Compensatory Mechanisms for Compressive Force Distribution • Contact area with knee flexion • Medial facet contact from 30-70 • Thickest hyaline cartilage in body
Compensatory Mechanisms for Compressive Force Distribution • Contact area with knee flexion • Medial facet contact from 30-70 • Thickest hyaline cartilage in body • Largest QF MA 30-70 • QF torque as MA decreases • QF tendon contacts condyles 70-90
Normal Patella Tracking • Maintains maximum congruence • Passive restraints • Active restraints
Abnormal Patella Tracking • ↓ congruence • Stretches capsule & retinacula • ↓ contact area Lateral Medial
Causes of Abnormal Tracking • Skeletal abnormalities • Strength imbalance in QF • Strength imbalance in fibrous tissues • Compensatory movements in knee due to abnormal foot movement
Causes of Abnormal Tracking • Skeletal abnormalities • Strength imbalance in QF • Strength imbalance in fibrous tissues • Compensatory movements in knee due to abnormal foot movement
Skeletal Abnormalities: Genu Varum & Genu Valgum • Q angle w/ age • Varum common in very young children • Valgum seen in growing children • Menisectomy effects
Skeletal Abnormalities: Patella Alta & Patella Baja • Index of Insall & Salviti • LT/LP • Normal = 1.0 • Patella alta = 0.8 • Patella baja = 1.2 • Women ratio
Skeletal Abnormalities: Patella Surface Lateral Border • Appositional forces ↓ in full extension • Prominence of lateral border prevents lateral displacement • Underdevelopment common in children as growing
Lateral tracking Skeletal Abnormalities: Femoral & Tibial Torsion
Causes of Abnormal Tracking • Skeletal abnormalities • Strength imbalance in QF • Strength imbalance in fibrous tissues • Compensatory movements in knee due to abnormal foot movement
Causes of Abnormal Tracking • Skeletal abnormalities • Strength imbalance in QF • Strength imbalance in fibrous tissues • Compensatory movements in knee due to abnormal foot movement