Download
1 / 34
340 likes | 596 Views
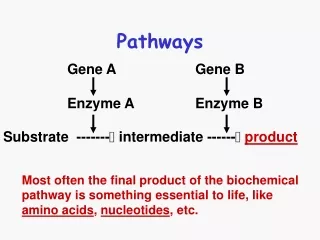
CUP Pathways. Dr Syed Zubair Consultant Medical Oncologist The James Cook University Hospital. Overview. Is CUP relevant and do we need pathways CUP pathways as recommended by NICE Real life CUP scenarios Local pathways. Is CUP relevant?.

E N D
CUP Pathways Dr Syed Zubair Consultant Medical Oncologist The James Cook University Hospital
Overview • Is CUP relevant and do we need pathways • CUP pathways as recommended by NICE • Real life CUP scenarios • Local pathways
Is CUP relevant? • In England: 9,778 new cases registered in 2006 (2.7%) • 4th most common cause of cancer death • No discrete classification within the ICD nomenclature • C77 to C80 usually cover registrations
Use of resources • HES (Hospital Episode Statistics) for England (06-07) • 25,318 episodes of care • 308,359 NHS bed-days • Admissions with CUP (2007): 365,197 patients • 72% as emergencies • 28% were elective admissions
Inpatient episodes • Inpatient episodes per 1000 population per year (2000 – 2007) • The highest rate was seen in the North East SHA.
Experience of patients • Lengthy diagnostic process with little new information discovered. • Disquiet at a string of investigations which may cause discomfort, adding little to care. • Confusion - who is in charge of care. • Long periods of inpatient stay with little perceived benefit. • Feel lack of fitting into a defined system when they meet other cancer patients. • Absence of an organised research programme.
Patient journey • Mr HR, 69 years old, previous history of prostate cancer on hormonal treatment • Presented to GP with intermittent dysphagia, clinically palpable nodes in the neck, • 2nd week July: Referred to Gastroenterology at North Tees • 18th July: OGD , soft tissue lesion around epiglottis • 20th July : Referred to ENT by GP • 25th July: Seen in ENT clinic, FNA of neck node • 4th Aug: Nasolaryngoscopy and Panendoscopy.No epiglottic lesions and normal larynx • 9th Aug: CT of TAP • 15th Aug: ENT clinic • 16th Aug: H&N MDT, NSC cancer, refer to upper GI MDT • 19th Aug : Upper GI MDT, PET and US core biopsy • 26th Aug: PET scan • 2nd Sep: Upper GI MDT, Radiological no evidence of upper GI cancer • 8th Sep: US guided neck node biopsy • 23rd Sep: Upper GI MDT, Likely CUP • 4th OCT H&N MDT: • 06th Oct: Combined clinic • 07th Oct: Referral to CUP team • 14th Oct : Seen in CUP clinic
confusing speculative unsure Defined CUP pathways Inconclusive equivocal ambiguous
Why are we still failing CUP patients? Lack of a system for clinical care Unknown Primary Cancer • No Specialist Oncologist • No Specialist Nurse • No Multi-disciplinary team • No MDT management approach • No Rapid systematic investigation • No Site-specific protocols • No Site-specific audit • No Site-specific research • No Cancer measures • No Site-specific information + support • No Accurate epidemiology Site-determined Cancer • Specialist Oncologist • Specialist Nurse • Multi-disciplinary team • MDT management approach • Rapid systematic investigation • Site-specific protocols • Site-specific audit • Site-specific research • Cancer measures • Site-specific information + support • Accurate epidemiology
Diagnosis and management of metastatic malignant disease of unknown primary origin Implementing NICE guidance July 2010 NICE clinical guideline 104
NICE Recommendations • Definitions • Epidemiology • Organisation of services and support • Diagnosis • Factors influencing management decisions • Managing specific presentations • Systemic treatment
Definitions Detection of metastatic malignancy on clinical examination or by imaging, without an obvious primary site MUO • Metastatic epithelial / neuro-endocrine malignancy on • histology. No primary detected despite initial investigations. Specialist review and possible further investigations pending pCUP Metastatic epithelial / neuro-endocrine malignancy on histology. Specialist review and all relevant investigations completed. No primary detected. cCUP
Organisation of CUP services • NSSG • Every hospital with a cancer centre or a cancer unit should establish • CUP team • CUP specialist nurse • Outpatients and inpatients with CUP • O/P : rapid referral pathway(2W). • I/P : assess by end of the next working day. • Local and Specialist CUP MDT
In patient referral • Mrs LK, 63, HT, Type 2 DM, PS-1 • Admitted to DMH, gen unwell, deranged BMS. • Pain in left arm, enlarged liver with abnormal LFTs • CT: Multiple liver mets, extensive nodal disease in abdo, lytic lesion in left humerus • Bone scan: Further uptake in right femur • USS guided liver biopsy: Mod diff adeno Ca, IHC unhelpful • Poor PS, palliative RT to left humerus and referral to palliative care team • Transferred to nursing home, For BSC
OPD referral • Mr CS, 60, accountant, IDDM, PS-0, chest team • Lumps in neck, headache and abnormal CXR • CT: disseminated malignancy with significant nodal mets, bilateral adrenal, liver, pulmonary, and cerebellar mets • Biopsy of neck node: poorly differentiated adenocarcinoma, extensive panel of IHC • Currently on palliative chemo
From Primary Care • Mrs JR, 63, PS-0, Fit, school supervisor • Dizzy spells and forgetting things • CT brain: 2 ring enhancing lesions in left temporal and one in the left parietal lobe – multiple brain mets • Staging CT: Possible lesion in Rt breast – workup NAD • MRI:Likely glioblastoma multiforme • Biopsy confirmed • Neurosurgical MDT: Ongoing discussions re - concurrent chemo radiotherapy or palliative radiotherapy
Concerns • IP/OPD: • Prolonged IP stay • Multiple investigations • Multiple MDTs • GP: • Who to refer • How far to investigate
Site specific cancer • Mrs PI, 49, PS-0, Fit and well, GP referral • 2-3 week h/o flashing lights and dizzy spells • CT Brain: 1 lesion in PO lobe and 2 in right frontal with extensive vasogenic oedema • No other sinister symptoms, stopped smoking in feb 20 cig/day • Staging CT: 34mm spiculated mass in LLL • Lung MDT: Radical appraocah ?gamma knife, further MRI brain at least 6 lesions • Rx: palliative chemo - PD after C2, Palliative RT to brain. ?2nd line Tarceva
Non cancer patients as CUP • Mrs GD, 54, lupus, ?osteoporosis,PS-0, via GP • Pain in cervical spine radiating down left arm, chronic intermittent pain LS spine • MRI: wide spread bony lesions in thoracic and lumbar spine consistent with bony mets • Staging CT: NAD • Bone scan : low grade uptake • Ankylosing spondylitis
Peer review • Primary care: current situation of referring to diagnosticians or MDTs • Pathway to start with diagnosis of MUO • NSSG in consultation with CUP MDT leads • Agree network-wide patient pathways (indication for referral, investigation and subsequent management) • Hospital specialists or A&E department • Acute Oncology • Pathways to include following specifications • Assessed face to face by a core member • OPD: R/v within 2 weeks of diagnosis of MUO • I/P: R/v by the end of next working day
CUP @ South NECN CUP service rolled out to • All patients from south NECN • JCUH / Friarage • Darlington / Bishop • North Tees / Hartlepool
CUP service will be rolled out for • All patients with a diagnosis of MUO/pCUP/cCUP • Imaging suggestive of metastatic malignancy with no obvious primary (no histology or cytology obtained) e.g. • multiple liver, lung, bone or brain metastases • Histology/cytology suggestive of carcinoma with no obvious primary on imaging
Outcomes of the CUP service • If PS 3 or more: Specialist palliative care. • cCUP: Assessment for systemic treatment. • Primary identified: Specialist MDT. • Non-malignant condition
Potential radical treatment • Squamous carcinoma upper or mid neck nodes • Head and neck MDT • Adenocarcinoma involving the axillary nodes • Breast cancer MDT • Squamous carcinoma confined to inguinal nodes • Specialist surgeon in an appropriate MDT • Solitary mets in liver/brain/lung • Appropriate MDT
CUP Diagnostic & Referral Pathways • Inpatient Pathway - Cancer Centre • Outpatient Pathway - Cancer Centre • Inpatient Pathway - Cancer Unit • Outpatient Pathway - Cancer Unit
CUP @ South NECN • Cancer Centre • CUP team • CUP MDT • Friday AM CUP clinic • Cancer Units • DMH/Bishop Auckland • Lead Clinician /AONS / Visiting Oncologist • North Tees/Hartlepool • Lead Clinician /AONS / Visiting Oncologist
Acknowledgements Dr Nicola Storey Nicky Hand
Thank you • Discussion