Download
1 / 37
390 likes | 728 Views
Osteoporosis – Controversies and Promising Treatment Options. Keith R. Holden, M.D. Ponte Vedra Beach, FL www.Dr-Holden.com. Osteoporosis Controversies. Guidelines for prevention and tx vary Bone quality versus bone quantity Same BMD can have different fx risk (age)

E N D
Osteoporosis – Controversies and Promising Treatment Options Keith R. Holden, M.D. Ponte Vedra Beach, FL www.Dr-Holden.com
Osteoporosis Controversies • Guidelines for prevention and tx vary • Bone quality versus bone quantity • Same BMD can have different fx risk (age) • Cumbersome dosing requirements • Drug side effects
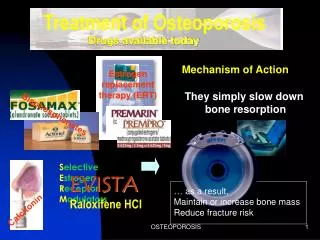
Bisphosphonate Side Effects • Esophagitis • Esophageal stricture • Esophageal cancer • Osteonecrosis of jaw • Atypical Femur Fracture
Atypical Femur Fracture (AFF) • Bisphosphonates ↓ osteoclast fxn & induce osteoclast apoptosis • Suppress bone resorption = hard, brittle bone • Path: ↓ bone heterogeneity = ↓ bone quality • Complete lack of TCN labeling = severe ↓ bone formation • Stress injury-like cortical hypertrophy in other femur with unilateral AFF
Limitations of BMD Tests (DEXA) • ↑ BMD does not always = ↑ bone strength • T-score not consistent predictor of osteoporosis outside of elderly postmenopausal white♀ • Other populations, Z score may be better predictor of low bone density
Fracture Risk Tool • www.shef.ac.uk/FRAX/tool.jsp • FRAX estimates 10-yr. fx risk based on BMD femoral neck + osteo risk factors
Bone Quality vs Bone Quantity • Bone quality = bone strength (cortical bone structure/quality of collagen) + rate of remodeling • Bone densitometry measures BMD (quantity), helps assess fx risk, aids in dx of osteo, but does NOT measure bone quality
Living Matrix of Bone • Healthy bone requires a balance of: • Bone building by osteoblasts • Resorption by osteoclasts
Osteoid Matrix of Bone • 90% collagen (majority Type 1) • Osteoclast degradation & osteoblast synthesis create circulating peptides of Type 1 collagen • Type I collagen is cross-linked by deoxypyridinoline (DPD) • DPD provides rigidity and strength (quality) to bone
Usefulness of Bone Biomarkers • Reflects bone remodeling yrs. before BMD ∆ • ↑ T score + ↑ biomarker → fx risk (odds 4.1) • Allow tracking of response to therapy • May improve adherence to therapy
Urinary Deoxypyridinoline (uDPD) • Cross-link Type IC (relatively selective) • Measure of bone resorption - ↑ urine level > bone loss • Unaffected by diet • Easy to measure spot AM urine • Recheck within 30-90 days after initiating therapy • Covered by Medicare
Effective Supplements for Bone • Calcium • Vitamin D • Magnesium • Boron • Strontium ranelate • Ipriflavone • Vitamin K • Choline stabilized orthosilicic acid (ch-OSA)
Choline stabilized orthosilicic acid • Ch-OSA = bioavailable silicon • RDBPC trial: added to calcium and D3 showing improved bone biomarkers and BMD ↑ 2% • RDBPC trial: ↑ tensile strength of hair • RDBPC trial: + effects of skin surface changes, mechanical properties, ↓ brittleness hair/nails
Biophysics and Bone Health • Pulsed Electromagnetic Field (PEMF) therapy has shown promise in clinical trials for tx and prevention of osteoporosis • Mediates process via cell signaling proteins – growth factors, cytokines, and prostaglandins
PEMF Improves BMD • PEMF 72Hz 10 hrs daily for 12 wks to radius of “osteoporosis prone” ♀ • BMD showed sig. inc. in exposed areas 36 wks • Similar but weaker response in non-treated arm (Tabrah, et. al., 1990)
PEMF Suppresses Bone Loss in DOP • Evaluated rats with surgically induced DOP • After 8 wks, PEMF sig. ↑BMD, ↑ TGF-beta 1, ↓IL-6 in proximal femur • Conclusion: PEMF efficiently suppresses bone loss in DOP via local factors (Shen, et al., 2010)
PEMF Chronotherapy in (OVX) rats • Evaluated CR with PEMF in ovariectomy-induced osteoporosis in rats • 12 weeks, (OVX-DPEMF) group had better prevention against OVX-induced bone loss • ↑BMD, ↑osteoblast activity, ↑ trabecular health markers; ↓bone markers of resorption (uDPD) (Jing, et. al., 2010)
PEMF ↓ DM Induced Bone Loss • Rats with streptozotocin-induced DM bone loss • PEMF daily 8 hrs x 8 wks • PEMF improved biomechanical bone quality DM bone • PEMF partially reversed DM-induced bone deterioration • Conclusion: PEMF might become an additive method for inhibiting DM osteoporosis (Jing, et al., 2011)
PEMF Affects Osteoblasts • Study on in-vitro osteoblastic cell culture • PEMF ↑osteoblastic growth, ↑ TGF-beta 1 • PEMF ↓ prostaglandin E2 • Conclusion: Study sheds light on mechanism of action of PEMF in non-union fx & prevention of osteoporosis (Li, et al., 2007)
PEMF Prevents Osteoporosis • Studied rats subjected to bil ovariectomy • PEMF augmented/restored trabecular bone mass/architecture in PEMF groups • PEMF attenuated higher serum PGE(2) of OVX rats and restored levels to that of controls • Conclusion: PEMF may be useful in prevention of osteoporosis resulting from ovariectomy (Chang, et al., 2003)
PEMF modulates osteoblast cells • PTH used to tx osteoporosis; Insulin & IGF-1 anabolic roles in osteogenesis • Cell signaling proteins IRS-1, S6 RSK, & eNOS were phosphorylated by PTH, Insulin, & PEMF to the same extent in osteoblast-like cells • Conclusion: Anabolic affects of PEMF may be mediated through these proteins (Schnoke, et. al., 2007)
Summary PEMF Physiologic Effects • ↑ BMD • ↑ TGF-beta 1 • ↓ IL-6 • ↓ PGE(2) • ↑ osteoblast growth • Phosphorylation of IRS-1, S6 RSK, eNOS
Use Food as Medicine • Alkalinizing plant based diet • Address food sensitivities • Mineral rich foods
Optimize Gut Health – 5Rs • Remove • Replace • Reinnoculate • Repair • Rebalance
Address Regulatory Blockades • Foci of interference (ANS) • Stress • Inflammation • Toxins • Allergy • Infection (occult, dysbiosis, dental) • Heavy metals
Supporting Factors • Resistance training • Nutritional supplementation • Hormonal balance • PEMF
Case Study #1 66 y.o ♀ with osteoporosis (T-score -3.1) • Baseline: mostly plant based diet, resistance training, Ca, Mg, and D • (1/27/11) uDPD 9.7 nM/mM Cr (NL < 6.5) • Weekly 1 hr PEMF sessions x 2 mos • (3/16/11) uDPD 4.5 (53% drop!) • Maintenance: Monthly 1 hr PEMF • (7/21/11) uDPD 5.5 • (10/24/11) uDPD 4.5
Case Study #2 63 y.o. ♀ osteoporosis (‘09 T-score LS -3.9; ‘11 T-score LS -4.1) • Hx FMG, CFS, IBS, MCS & hx multiple fxs • Baseline: BHRT, Ca, Mg, D • Added ch-OSA + tx gut dysbiosis • Started PEMF (3/26/11) monthly; (7/26/11) inc. freq. to weekly; (9/12/11) 2-3 X week • (4/13/11) uDPD 9.7; (10/4/11) uDPD 5.0 (48.45% drop!)
Contact Information Keith R. Holden, M.D. 822 A1A North, Suite 310 Ponte Vedra Beach, FL 32082 (904) 473-4954 krholden@gmail.com www.Dr-Holden.com