Download
1 / 2
20 likes | 155 Views
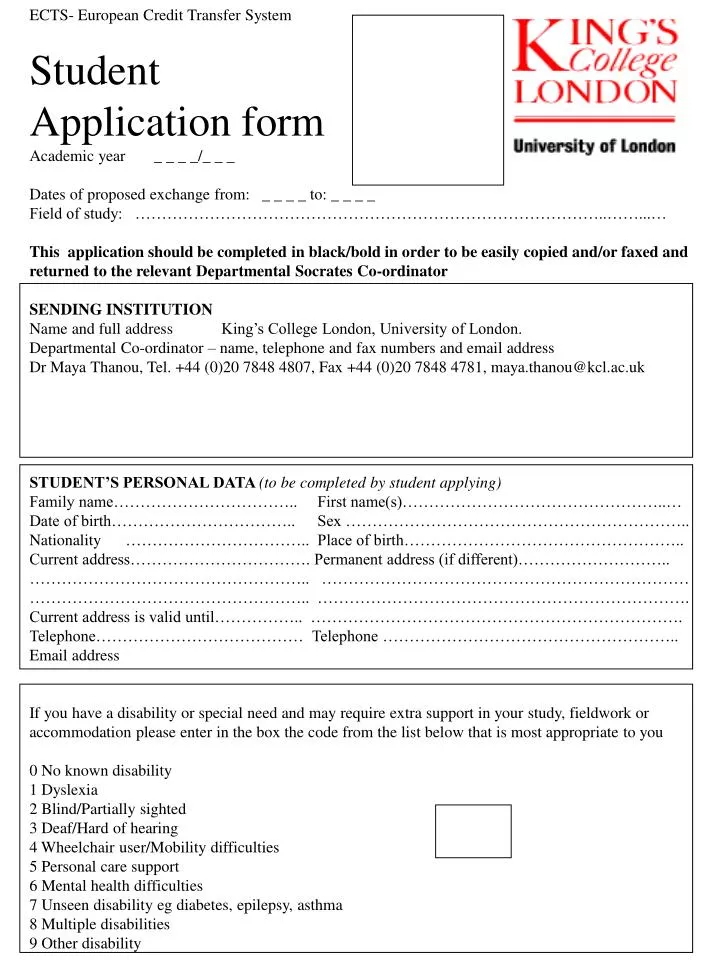
ECTS- European Credit Transfer System Student Application form Academic year _ _ _ _/_ _ _ Dates of proposed exchange from: _ _ _ _ to: _ _ _ _ Field of study: ……………………………………………………………………………..……...…

E N D
ECTS- European Credit Transfer System Student Application form Academic year _ _ _ _/_ _ _ Dates of proposed exchange from: _ _ _ _ to: _ _ _ _ Field of study: ……………………………………………………………………………..……...… This application should be completed in black/bold in order to be easily copied and/or faxed and returned to the relevant Departmental Socrates Co-ordinator SENDING INSTITUTION Name and full address King’s College London, University of London. Departmental Co-ordinator – name, telephone and fax numbers and email address Dr Maya Thanou, Tel. +44 (0)20 7848 4807, Fax +44 (0)20 7848 4781, maya.thanou@kcl.ac.uk STUDENT’S PERSONAL DATA (to be completed by student applying) Family name…………………………….. First name(s)…………………………………………..… Date of birth…………………………….. Sex ……………………………………………………….. Nationality …………………………….. Place of birth…………………………………………….. Current address……………………………. Permanent address (if different)……………………….. …………………………………………….. …………………………………………………………… …………………………………………….. ……………………………………………………………. Current address is valid until…………….. ……………………………………………………………. Telephone………………………………… Telephone ……………………………………………….. Email address If you have a disability or special need and may require extra support in your study, fieldwork or accommodation please enter in the box the code from the list below that is most appropriate to you 0 No known disability 1 Dyslexia 2 Blind/Partially sighted 3 Deaf/Hard of hearing 4 Wheelchair user/Mobility difficulties 5 Personal care support 6 Mental health difficulties 7 Unseen disability eg diabetes, epilepsy, asthma 8 Multiple disabilities 9 Other disability Student’s signature……………………………………………….. Date…………………………….. SENDING INSTITUTION We confirm that this proposed programme of study/learning agreement is approved. Departmental Co-ordinator’s signature Date Institution co-ordinator’s signature Date ……………………………………………………………………………………………………………. RECEIVING INSTITUTION We confirm that this proposed programme of study/learning agreement is approve. Departmental Co-ordinator’s signature Date Institution co-ordinator’s signature Date …………………………………………………………………………………………………………….
Briefly state the reasons why you wish to study abroad……………………………………………… ……………………………………………………………………………………………………..………………………………………………………………………………………………………………... LANGUAGE COMPETENCE Mother tongue ……………………………………………………………………………………….. Language of instruction at home institution (if different) ................................................................. I am currently studying the English language I have sufficient knowledge to follow lectures I have taken an English language test eg IELTS, TOEFL Title of test, result, date ……………………………………………………………………………. I intend taking an English language test Title of test, result, date ……………………………………………………………………………. PREVIOUS AND CURRENT STUDY Diploma/degree for which you are currently studying Number of higher education study years prior to departure abroad Have you already studies abroad? If yes, at which institutions? .............................................................................................................. The attached Transcript of records includes full details of previous and current higher education study. Details not known at the time of application will be provided at a later stage RECEIVING INSTITUION I hereby acknowledge receipt of the application, the proposed Learning Agreement and the Candidate’s Transcript of records. I confirm that the Learning Agreement has been completed and signed by all necessary signatories and that the student should be made a formal offer to study in my department from …………………………………to……………………….……………….. Departmental Co-ordinator’s signature………………………………………………………………. Date…………………………………………………………………………………………………… Yes: No: Yes: No: Yes: No: Yes: No: Yes: No: