Download

1 / 61
610 likes | 760 Views
Integrated Care Manager Training. Integrated Care Manager (ICM) Training. CONTENTS Integrated Care – what are we talking about? Older People’s needs Case Management in General Practice Enabling Integrated Care Managers Concerns About Older People. The Vision.

E N D
Integrated Care Manager (ICM) Training • CONTENTS • Integrated Care – what are we talking about? • Older People’s needs • Case Management in General Practice • Enabling Integrated Care Managers • Concerns About Older People
The Vision Healthier, happier and longer lives through a radical transformation of how professionals and communities work together to provide integrated care and better value, with empowered citizens better able to look after themselves through supported self care.
Southwark and Lambeth Integrated Care : a federation of health and social care organisations and communities supported by GSTT Charity
The Mission Build community with assets, capabilities and skills to support self care. 1. • Ensure that people in Southwark and Lambeth reliably receive the right care in the right place at the right time. 2. • Ensure that we are treating the whole person with care centred around the empowered individual. 3. • Ensure professionals are best able to deliver this new approach. 4. • Ensure better professional lives for the staff we are working with. 5.
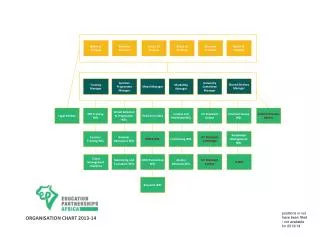
What is our joined-up approach? Redesign services and care pathways A new system where we all think and work together differently IT & informatics How & what organisations are paid Governance across participating organisations Workforce & change in practice Holistic care: Older people Long-term conditions in working-age adults Engaging citizens, patients and staff
ICM Training • CONTENTS • Integrated Care – what are we talking about? • Older People’s needs • Case Management in General Practice • Enabling Integrated Care Managers • Concerns About Older People
Integrated care for older people is our first priority • Older people told us they want: I want to stay fit and healthy I want to stay out of hospital or care home for as long as I can I want to have longer to talk about my needs with someone who understands I want all my needs looked at – including my mental health If I have to go to hospital, I want to be assessed quickly and return home
What are the key changes for older people’s care? • An holistic system to help people with complex needs • Identifying needs through risk stratification and ‘holistic health assessment’ • Case management • Community-based multidisciplinary team • Increased access to reablement • Support for earlier intervention on falls, infection, nutrition and dementia • Better urgent response • Telephone advice for GPs, ICMs, practice nurses, community matrons and social workers • Bookable ‘hot clinics’ • ‘Home ward’ and rapid response teams to avoid admission • Simplified hospital discharge process
Benefits of Older People’s Programme Benefits as outlined within Integrated Care Programme Charity Bid Business Case signed off by Programme Board and Sponsor Group in Autumn 2011 End of year 3
ICM Training • CONTENTS • Integrated Care – what are we talking about? • Older People’s needs • Case Management in General Practice • Enabling Integrated Care Managers • Concerns About Older People
Case Management in general practice • Overview of case management • Overview of Integrated Care Manager role • Outcomes of ICM role • Activities of an ICM • Caseload management Southwark & Lambeth Integrated Care
OVERVIEW OF CASE MANAGEMENT- Definitions • What is Case Management? • Hutt et al (2004) described it as: • ‘The process of planning, co-ordinating and reviewing the care of an individual’. • The Case Management Society of America (CMSA)- where case management has been in place for some time- defines it as: • ‘A collaborative process of assessment, planning, facilitation, care coordination, evaluation, and advocacy for options and services to meet an individual’s and family’s comprehensive health needs through communication and available resources to promote quality cost-effective outcomes’ (CMSA website). http://www.cmsa.org/
OVERVIEW OF CASE MANAGEMENT- Rationale • The DoH have highlighted case management as a key component of effective management of people with complex needs, with the key aims of: • Improving the experience of the individual and their family • Improving the outcomes for the individual being case managed and their family • Reducing hospital admission (particularly emergency admissions) • The complexity of peoples’ needs (health and social care) may result from a single condition or situation, but is more likely to be the result of more than one condition, and/ or social situation.
Community Matron 2,000 people covered per year Coverage of Case Managers in Lambeth & Southwark Case Managers 3000 ‘new’ older people covered per year Integrated Care Manager
OVERVIEW OF CASE MANAGEMENT- Activities Assessment and re-assessment Case finding Case Management Care / action planning Care co-ordination Self care support Review
See Handout- JD Required Outcomes of ICM Role • Outcomes for the person being case managed: • Maximisation of independence • Move towards self care • Sign posting to appropriate services (including in the voluntary sector) • Process outcomes: • Review of all current care plans and medications • Identification of actions to be taken to improve the person’s health and well being • An agreed health and social care action plan
Who will be case managed? • The decision to case manage someone will be a matter for professional and clinical judgement, as will the decision on the level of case management required. However the following criteria are likely to be relevant to these decisions: • Have complex needs • Are at risk of admission to hospital • Are at risk of placement in a care home • Need interventions from a number of different services • Have particular combination of needs with his/her spouse/partner and/or family • Are the in the top 10 per cent of those at risk on PHMCC register • Where the specific management/care plan(s) in place already (e.g. under a diabetes nurse) does not meet all needs and/or manage all risks • The person themselves, or their carer, thinks that case management would be useful.
Activities: Case Finding • Within the context of the SLIC, case finding will be done by: • Community matrons • Practice staff carrying out the Holistic Health Assessment • In the short to medium term, ICMs will also find cases by: • Discussing with practice staff any people they currently know who could benefit • Reviewing GP system data for emergency admissions • Reviewing risk stratification software (PHMCC) • Reviewing ICP Register information in Practice Focus
Activities: Assessment and Re-assessment • Consists of: • Review of all current care plans and discussion with the relevant health and social care professionals • Mapping of social networks • Review of medical notes (or ensuring it is done) • Medications review (or ensuring it is done) • Discussing current care with the person being case managed to identify what is and is not working and what the person’s personalised goals are • Co-produced approach with the person • Requires informed explicit consent for sharing information
Activities: Care / Action Planning • For ICMs this will consist of: • Discussion with the person being case managed about their required personal outcomes • Discussion of the person’s care at the Community Multi Disciplinary Team Meeting (CMDT) if appropriate/relevant • Developing and agreeing an action plan that outlines: • What actions will be taken • Who is responsible • Timescale for action • Expected outcomes
Activities: Care Coordination • Key activity of case management and requires: • Effective communication with person being case managed and their carers/family • Effective communication with health and social care professionals working with the person • Development of trust between case manager and case managed- advocacy and negotiation • Sign posting to other services - including voluntary sector organisations
Activities: Self Care Support • Self care support includes a range of activities, for example: • Health promotion • Referrals for specific issues/ conditions or to specific schemes e.g. to a dietician, consultant or clinic; to self-care programmes e.g. Expert Patient • Sign-posting to appropriate services (including voluntary sector organisations) • Referral to services for maximisation of all benefits • Referral to reablement services • Provision of assistive technology and community equipment • Provision of a community alarm service
Activities: Review • The ICM reviews whether the actions outlined in the action plan have been achieved, and if not identifies reasons • Follows up with other health and social care professionals where appropriate • Sets appropriate timescale for further review, may result in the person being discharged from case management
Caseload Management • Key processes to ensure caseloads are manageable Selecting the right people (where you can make a difference) Initial assessment (identifying the key issues) Identifying goals (to track progress) Support & advice from the CMDT and its members Reviewing people (eg, when ‘short term’ becomes ‘long term’) Discharging people (Have goals been met? Is the plan working?) Correct coding of your activity (to ensure you can monitor your caseload & that payment information is accurate) • CMDTs and the Integrated Care Operations Board will monitor activity levels and welcome feedback on how well your role is working
ICM Training • CONTENTS • Integrated Care – what are we talking about? • Older People’s needs • Case Management in General Practice • Enabling Integrated Care Managers • Concerns About Older People
Enabling ICMs • CMDTs • Integrated Action Plan • IT support and management • Information governance & consent • Payment structure & Read Codes • Quality & activity monitoring • Clinical Lead role in your practice & you • Induction & introducing yourself • Medicines management • Telephone numbers Southwark & Lambeth Integrated Care
CMDTs and ICMs • CMDT overview • CMDT Chair • CMDT clinical meeting • CMDT governance meeting • CMDT referral process and meetings
What is the community multi-disciplinary team? • Supporting case management • clinical meetings every 2 weeks • Improving the quality of care for local people • governance (quality review) meetings every 2 months Admin and IT support
CMDT Overview • 6 CMDTs across Lambeth and Southwark: one CMDT in each Locality • Each meeting planned to last 2 hours • Core membership of clinical CMDT does not include all ICMs • ICM or general practice represented at clinical CMDTs when patient from that practice is discussed • Every general practice must be represented at Quality Review (Governance) CMDTs
The CMDT Chair • All CMDTs will have a chair who is responsible for: • Building and developing the capability of the CMDT • Leading the CMDT clinical and quality review / governance meetings • Holding CMDT members to account for delivering integrated action plans • Encouraging creative problem solving • Enabling CMDT members to reach solutions • Leading and supporting service or system improvements • Negotiating across organisational boundaries to achieve service or system improvements • Representing their Locality at the ICP Operations Board
CMDT clinical meeting • CMDT members will: • Maximise existing local expertise • Contribute to the development and delivery of integrated action plans • Challenge existing practice • Unblock bottle necks to access appropriate services • Monitors progress • Support effective communication within their organisation
CMDT Quality Review / Governance meetings • CMDT members will: • Review past performance through case audits • Cascade learning across their team and organisation • Recommend system improvements • Support the implementation of system improvements
Referring to CMDTs • Email lead administrator (see emails on last slide) • Ask for referral process and when meeting dates are • Complete a ‘Case Summary Template’ (see next slide)
See Handout – case summary template Referring to CMDT – Case summary template
See Handout - IAP Integrated Action Plan • The Integrated action plan (IAP) is a tool to support case management as it enables information from multiple sources to be structured and kept in one place • It is a word document that is now a template on Practice Focus • The IAP uploads information from your GP system about your patient • It can’t download information • It can be saved, edited and shared, and eventually saved as a pdf and attached to the patient’s notes Tip: In Practice Focus, under ‘Local Audit’ click on ‘ICP Older People’ button, and the IAP is at top of screen
IAPs – do’s and don’ts • Do let us know how you get on using it • Don’t share it via email unless you know who you are sharing it with – watch out for attaching it to ‘reply all’ • Do summarise • Do check patient consent for sharing information – there is a tick box in the IAP if patient has consented to share information and it is not being displayed in the uploaded information • Don’t print it all out unless you have to – it’s designed as an electronic document
IT Support and Management A ‘blended’ approach for IT…. • Principles for IT: • Pragmatic • Scalable • Cost Effective • Timely • Leading Edge Including Collaborator Adopting an explicit consent model – initiated from incoming referral
Information governance and consent • You are to use your practice’s information governance (IG) policy in your work • You need to check that the patient has explicitly consented that her/his information can be shared with you and with other health and social care professionals • If the patient has had a HHA (and has been invited using a letter with the correct IG words in it) then the patient has explicitly consented to sharing her/his records • If you are unsure, then you need to check. • These are the relevant Read Codes: • 9Ndl - Implied Consent (core data only) • 9Ndm - Express Consent (core data only) • 9Ndn - Express Consent (core data & additional info) • 9Ndo - Express Dissent (If the patient does not want a Summary Care Record)
These codes used to triggerpayment Length ofIntervention ICM payment structure & Read Codes Referral received Initial scan for suitability Timestamp: 8CV0 “Case management started” Collate data Decision: 9NNL “Under care of case manager” (PROCEED) Or 8Hkj. “Informal referral-signposted to other agency” (STOP) Or 9Ng0 (“Assessed as not suitable for case mgt.” (STOP) Develop action plan Timestamp: 8CS2 “Health & social care plan agreed” Deliver action plan Timestamp: 8CT0 “Case management ended”
Quality & Activity Monitoring • Information on activity and outcomes will be reported to CMDTs as part of their governance and quality review role • Outcome measures include emergency admissions & attendances, residential care admissions, older people supported to live at home and people’s views about their care & support • Key measures relevant to integrated case management • Caseload • Length of stay (LT v ST cases) • % with agreed care plan in place • % new referrals not suitable/referred to other agencies instead • Measures under development • % of people who received integrated case mgt in last 6 months who since attended ED/were admitted in an emergency • Case file audits of case management
Integrated Care Clinical Lead in your practice • The Clinical Lead has a responsibility to support you • This is quoted from the LES contract, Appendix 1 page 2: • ‘I will ensure that the Primary Care Case Manager (now the Integrated Care Manager) is supported in her/his role, which includes ensuring that she/he is supported to represent the practice in all discussions at CMDT meetings and in relation to any follow-up action needed in the practice’ • Your clinical lead has agreed to do this
Induction • In order to carry out your role you need to know people in your host practice and in the organisations you are working with. Examples include: • Core Community Multi disciplinary team members: • CMDT Chair • Community Matrons • Other Integrated Care Managers • Therapy lead • Social care lead • Mental health lead • Care of the elderly lead • Local health and social care support agencies After you’re trained, go to the first available CMDT to meet partners
See Handout - leaflet Introducing yourself • We have drafted a leaflet for you to use to introduce yourself to people on your caseload • Please tell us what you think of the leaflet • Some of the words in it may help you to explain your role
See Handout – slide pack Medicines management • Medicines and Integrated Care • ICM medicines tool • ICM questions • Medicines issues • Community pharmacist contact details
Medicines and Integrated Care • One criterion for being included on the Integrated Care register is: “Is the person on four or more medications including one of six medicines with the highest risk of hospital admission (insulin, warfarin, NSAIDs, digoxin, diuretics and antipsychotics)?” Because evidence shows that people with this profile are more likely to have an avoidable admission • Holistic Health Assessment asks: • Has patient had a medicine review within the last year? • If yes, then do nothing, if no, then refer to GP for a medicine review