Download
1 / 41
420 likes | 645 Views
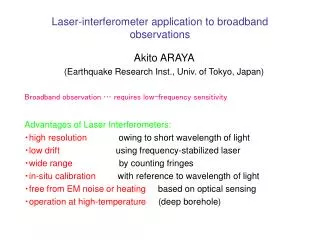
Endobronchial Laser Application. Bernward Passlick Professor of Thoracic Surgery Dept. of Thoracic Surgery University Medical Center Freiburg, Germany. Palliative treatment/ Recanalisation. With potentially curative Intent. Indications for Endobronchial Laser Applications.

E N D
Endobronchial Laser Application Bernward Passlick Professor of Thoracic Surgery Dept. of Thoracic Surgery University Medical Center Freiburg, Germany
Palliative treatment/Recanalisation With potentiallycurative Intent Indications for Endobronchial Laser Applications Bollinger CT et.al. Eur J Resp (2006) 27: 1258
Historical Developments 1976 first endobronchial laser resection with a CO2 Laser 1978 first endobronchial treatment with a Neodym YAG - Laser ( wave length 1064nm / depth 5 mm) 1982/1983 first publications in Germany about endobronchial laser application( Dierkesmann / Häussinger) 1988 first publication about the experience of more than 1000 patients 2001 MY 40 YAG Laser (wave length 1312 nm / depth 5-10 mm) 2010 Limax 60/120 Laser System
Different Laser Types Modidfied from: Bollinger CT et.al. Eur J Resp (2006) 27: 1258 - 1271
Current laser system: Limax Limax 60/ Limax 120: • 1-60W or 1-120W of power • Diode pumped Nd:YAG-Laser • Integrated smoke evacuator • Integrated gas flow • Lung parenchyma and endobronchial application
Practical Setting Use of the laser with rigid or flexible bronchoscopes Almost always combination of both Laser application always in narcosis Jet ventilation via rigid scope Power Setting 15-25 W, pulse duration: continuos mode
Palliative treatment/Recanalisation Indications for Endobronchial Laser Applications Bollinger CT et.al. Eur J Resp (2006) 27: 1258
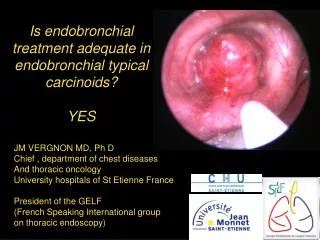
Palliative Treatment and Recanalisation Symptomes (n =110) • Patientswith: • End stagetumorrecurrences • Failedchemoradiation • UnrecognizedMetastasesor Primary Tumors After Han C et.al. J Thorac Oncol (2007) 2: 50 -64.
Basic Types of Central Airway Stenosis Bollinger CT, Eur. Respir J., 2006
Different exampels of endobronchial stenosis Mixed endoluminal extraluminal
Mixed Central Airway Stenosis The aimisrecanalisation!
Techniques of endobronchial recanalisation Mechanical: debulking with a forceps ( flexible, optical forceps; rigid tube) Argon beamer: coagulation of the tumor surface • Alternative: LASER DESOBLITERATION
Success rate of laser assisted recanalisation relation to the location of the tumor 88% 85% 90% 76% 74% 44% 62% 80% 70% 50% Huala K. et. al. Eur Arch Otorhinolaryngol (2003) 260:219-222
10 Golden Rules of Safe ND:YAG Laser Resection Know the anatomic danger zones: aortic arch, pulmonary artery and esophagus being the main hazard areas Have a well-trained laser team, including an experienced anesthesiologist Screen patients carefully: purely external compression is beyond the reach of the technique Use the rigid bronchoscope technique for any high-grade obstruction, especially if malignancy is involved Monitor blood gases and cardiac performance. At least sign of hypoxemia, interrupt treatment long enough to oxygenate the patient
10 Golden Rules of Safe ND:YAG Laser Resection Fire the laser parallel to the wallof the airway; never aim directly to it Coagulate at will but avoid using the laser at high power settings Do not neglect hemorrhage, for even slow bleeding will lead to hypoxemia if left unattended Terminate each procedure with a tracheobronchial toilet to remove all secretions and/or debris Keep the patient under observationin a special room for a reasonable period of time
Case Report: Endobronchial metastases Endobronchial Laser Application
Endoluminal Stenosis:Squamous cell carcinoma of the trachea Endotracheal polypoid tumor
Endoluminal stenosis:Squamous cell carcinoma of the trachea Tumor resection by a rigid bronchoscope
Endoluminal stenosis:Squamous cell carcinoma of the trachea Laser treatment of the tumor basis
Endoluminal stenosis:Squamous cell carcinoma of the trachea Final result
Long term survival after Laser desoblitaration N = 89 Huala K.et.al. Eur Arch Otorhinolaryngol (2003) 260: 219 – 222.
Treatment of mixed Central Airway Stenosis Endobronchial situation
Treatment of mixed Central Airway Stenosis Laser recanalisation
Treatment of mixed Central Airway Stenosis Situation after implantation of a bifurcation stent
Typical carcinoid tumor: Preoperative recanalisation Initial CT scans
Typical carcinoid tumor: Preoperative recanalisation UL Complete obstruction of the lower lobe bronchus Bronchoscopy: Initial findings
Typical carcinoid tumor: Preoperative recanalisation Laser-dissected part of the tumor Tumor basis Präoperative Recanalisation
Segment-6 sleeve resection after preoperative recanalisation S6 S10 S8-9 Resection margins „Neo-Carina“ S8-9/10; Running Suture dorsal part (PDS 5-0) Single suture ventral part
Segment-6 sleeve resection after preoperative recanalisation OL Anastomosis Seg. 8,9,10 Bronchoscopy: 3 months postoperatively
With potentiallycurative Intent Indications for Endobronchial Laser Applications Bollinger CT et.al. Eur J Resp (2006) 27: 1258
Benign stenosis due to Tracheal Papillomatosis Situation after laser resection
Benign stenosis due to Tracheal Papillomatosis Tracheal Papilloma prior Laser resection Tracheal Papilloma 2 weeks after Laser resection
Basic Types of non-tumor-related Tracheal Stenoses Web like stenosis; Tracheal wall preserved Sand clock stenosis; Tracheal wall destroyed
Web-like Tracheal stenosis Laser-Incision of a post intubation Web-like Lesion
Summary Relevant tracheobronchial stenosis are a common clinical problem Assessment: Chest CT when ever possible Rigid bronchoscope + experienced anaesthesiologist Determine the type and localization of bronchial stenosis Aim is the complete recanalisation Morbidity and mortality after laser resection is low Modern laser systems allow different applications in lung parenchyma surgery and endobronchial applications