Download
1 / 1
10 likes | 878 Views
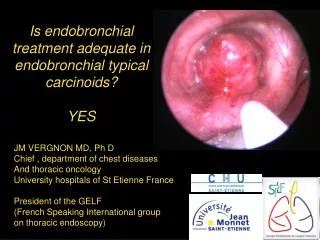
Georgetown University Endobronchial Brachytherapy Stent Farshid Firoozbakht, MD, MPH 1 ; David Duhamel, MD 2 ; Derick Hanlan, MD 2 ; John Feigert, MD 2 .

E N D
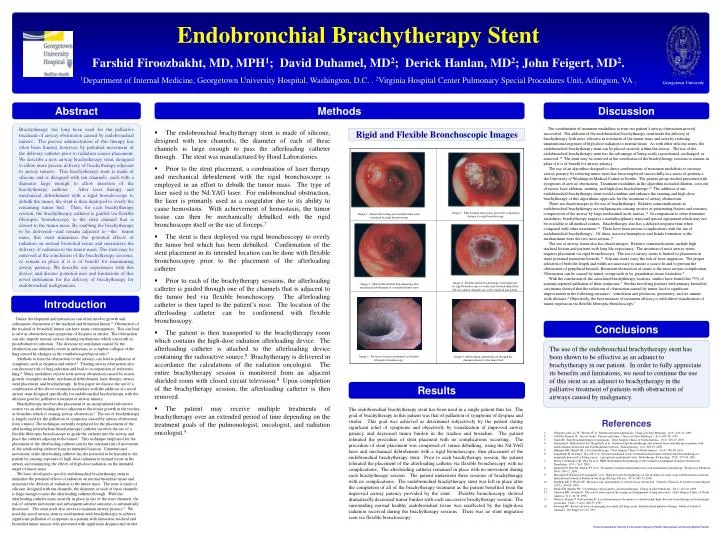
Georgetown University Endobronchial Brachytherapy Stent Farshid Firoozbakht, MD, MPH1; David Duhamel, MD2; Derick Hanlan, MD2; John Feigert, MD2. 1Department of Internal Medicine, Georgetown University Hospital, Washington, D.C. . 2Virginia Hospital Center Pulmonary Special Procedures Unit, Arlington, VA . Abstract Methods Discussion The combination of treatment modalities to treat our patient’s airway obstruction proved successful. The addition of the endobronchial brachytherapy stent made the delivery of brachytherapy both more effective in treatment of the tumor mass and safer by reducing unintentional exposure of high-dose radiation to normal tissue. As with other silicone stents, the endobronchial brachytherapy stent can be placed securely within the airway. The use of the endobronchial brachytherapy stent has the advantage of being easily repositioned, exchanged, or removed.10 The stent may be removed at the conclusion of the brachytherapy sessions or remain in place if it is of benefit for airway patency. The use of an algorithm designed to direct combinations of treatment modalities to increase airway patency by reducing tumor mass has been employed successfully in a series of patients a the University of Washington Medical Center in Seattle. The patient group studied presented with symptoms of airway obstruction. Treatment modalities in the algorithm included dilation, core-out of tumor, laser ablation, stenting, and high-dose brachytherapy.10 The addition of our endobronchial brachytherapy stent would combine and enhance the stenting and high-dose brachytherapy of this algorithmic approach for the treatment of airway obstruction. There are disadvantages to the use of brachytherapy. Relative contraindications to endobronchial brachytherapy are malignancies causing erosive or penetrating lesions and extrinsic compression of the airway by large mediastinal node masses.14 In comparison to other treatment modalities, brachytherapy requires a multidisciplinary team and special equipment which may not be available at all medical centers. Brachytherapy also has a delayed response time when compared with other treatments.14 There have been serious complications with the use of endobronchial brachytherapy. Of these, massive hemoptysis and fistula formation to the mediastinum were the two most serious.11 The use of airway stents also has disadvantages. Relative contraindications include high tracheal lesions and patients with long life expectancy. The insertion of most airway stents requires placement via rigid bronchoscopy. The use of airway stents is limited to placement in more proximal mainstem bronchi.14 Silicone stents carry the risk of stent migration. The proper selection of both the length and width are necessary to ensure a secure fit and to prevent the obstruction of peripheral bronchi. Recurrent obstruction of stents is the most serious complication. Obstruction can be caused by tumor overgrowth or by granulation tissue formation.2 With the conclusion of the calculated brachytherapy sessions, studies have found that 75% of patients reported palliation of their symptoms.7 Studies involving patients with primary bronchial carcinoma showed that the reduction of obstruction caused by tumor lead to significant improvement in the following measures: ventilation and perfusion, spirometry, and six minute walk distance.8 Objectively, the best measure of treatment efficacy is with direct visualization of tumor regression via flexible fiberoptic bronchoscopy.7 Brachytherapy has long been used for the palliative treatment of airway obstruction caused by endobronchial tumors. The precise administration of this therapy has often been limited, however, by potential movement of the delivery catheter prior to radiation source placement. We describe a new airway brachytherapy stent, designed to allow more precise delivery of brachytherapy adjacent to airway tumors. This brachytherapy stent is made of silicone and is designed with ten channels, each with a diameter large enough to allow insertion of the brachytherapy catheter. After laser therapy and mechanical debridement with a rigid bronchoscope to debulk the tumor, the stent is then deployed to overly the remaining tumor bed. Then, for each brachytherapy session, the brachytherapy catheter is guided via flexible fiberoptic bronchoscopy to the stent channel that is closest to the tumor mass. By enabling the brachytherapy to be delivered—and remain adjacent to—the tumor mass, this stent minimizes the potential effects of radiation on normal bronchial tissue and maximizes the delivery of radiation to the tumor mass. The stent may be removed at the conclusion of the brachytherapy sessions, or remain in place if it is of benefit for maintaining airway patency. We describe our experiences with this device, and discuss potential uses and limitations of this novel instrument for the delivery of brachytherapy for endobronchial malignancies. • The endobronchial brachytherapy stent is made of silicone, designed with ten channels, the diameter of each of these channels is large enough to pass the afterloading catheter through. The stent was manufactured by Hood Laboratories. • Prior to the stent placement, a combination of laser therapy and mechanical debridement with the rigid bronchoscope is employed in an effort to debulk the tumor mass. The type of laser used is the Nd:YAG laser. For endobronchial obstruction, the laser is primarily used as a coagulator due to its ability to cause hemostasis. With achievement of hemostasis, the tumor tissue can then be mechanically debulked with the rigid bronchoscope itself or the use of forceps.5 • The stent is then deployed via rigid bronchoscopy to overly the tumor bed which has been debulked. Confirmation of the stent placement in its intended location can be done with flexible bronchoscopoy prior to the placement of the afterloading catheter. • Prior to each of the brachytherapy sessions, the afterloading catheter is guided through one of the channels that is adjacent to the tumor bed via flexible bronchoscopy. The afterloading catheter is then taped to the patient’s nose. The location of the afterloading catheter can be confirmend with flexible bronchoscopy. • The patient is then transported to the brachytherapy room which contains the high-dose radiation afterloading device. The afterloading catheter is attached to the afterloading device containing the radioactive source.8 Brachytherapy is delivered in accordance the calculations of the radiation oncologist. The entire brachytherapy session is monitored from an adjacent shielded room with closed circuit television.8 Upon completion of the brachytherapy session, the afterloading catheter is then removed. • The patient may receive multiple treatments of brachytherapy over an extended period of time depending on the treatment goals of the pulmonologist, oncologist, and radiation oncologist.4 Rigid and Flexible Bronchoscopic Images Image 2: Mid-tracheal tumor mass post laser coagulation therapy via rigid bronchoscopy. Image 1: Initial obstructing mid-tracheal tumor mass visualized by rigid bronchoscopy. Image 4: Endobronchial brachytherapy stent deployed via rigid bronchoscopy to overly mid-tracheal tumor bed. All ten catheter channels are well-visualized and patent. Image 3: Mid-tracheal tumor bed remaining after mechanical debridement of coagulated tumor mass. Introduction Tumor development and metastases can often involve growth and subsequent obstruction of the tracheal and bronchial lumen.8 Obstruction of the tracheal or bronchial lumen can have many consequences. This can lead to airway obstruction and symptoms of dyspnea or stridor. The obstruction can also impede normal airway clearing mechanisms which can result in postobstructive infection. The decrease in ventilation caused by the obstruction can ultimately result in atelectasis or complete collapse of the lung caused by changes in the ventilation-perfusion ratio.8 Methods to treat the obstruction of the airways can lead to palliation of symptoms such as dyspnea and stridor.3 Treating airway obstruction also can decrease risk of lung infection and lead to re-expansion of atelectatic lung.8 Many modalities exist to treat airway obstruction caused by tumor growth, examples include: mechanical debridement, laser therapy, airway stent placement, and brachytherapy. In this paper we discuss the use of a combination of the above treatment modalities with the addition of a novel airway stent designed specifically for endobronchial brachytherapy with the ultimate goal for palliative treatment of airway tumors. Brachytherapy involves the placement of an encapsulated radioactive source via an afterloading device adjacent to the tumor growth in the trachea or bronchus which is causing airway obstruction.1 The use of brachytherapy is largely used for the palliation of symptoms caused by airway obstruction from a tumor. The technique currently employed for the placement of the afterloading polyethylene (brachytherapy) catheter involves the use of a flexible fiberoptic bronchoscope to guide the catheter into the airway and place the catheter adjacent to the tumor.1 This technique employed for the placement of the afterloading catheter carries the constant risk of movement of the afterloading catheter from its intended location. Unintentional movement of the afterloading catheter has the potential to be harmful to the patient by causing exposure of high-dose radiation to normal tissue in the airway and minimizing the effects of high-dose radiation on the intended target of tumor mass. We have developed a specific endobronchial brachytherapy stent to minimize the potential effects of radiation on normal bronchial tissue and maximize the delivery of radiation to the tumor mass. The stent is made of silicone, designed with ten channels, the diameter of each of these channels is large enough to pass the afterloading catheter through. With the afterloading catheter more securely in place in one of the stent channels, the risk of catheter movement and subsequent adverse outcomes is substantially decreased. The stent itself also serves to maintain airway patency.2 We used this novel airway stent in combination with brachytherapy to achieve significant palliation of symptoms in a patient with metastatic tracheal and bronchial tumor masses who presented with significant dyspnea and stridor. Conclusions The use of the endobronchial brachytherapy stent has been shown to be effective as an adjunct to brachytherapy in our patient. In order to fully appreciate its benefits and limitations, we need to continue the use of this stent as an adjunct to brachytherapy in the palliative treatment of patients with obstruction of airways caused by malignancy. Image 5: Position of stent reconfirmed via flexible fiberoptic bronchoscopy. Image 6: Afterloading catheter placed through the channel adjacent to the tumor bed. Results The endobronchial brachytherapy stent has been used in a single patient thus far. The goal of brachytherapy in this patient was that of palliation of symptoms of dyspnea and stridor. This goal was achieved as determined subjectively by the patient stating signifcant relief of symptoms and objectively by visualization of improved airway patency and decreased tumor burden in the trachea and bronchus. The patient tolerated the procedure of stent placment with no complications occurring. The procedure of stent placement was comprised of: tumor debulking using the Nd:YAG laser and mechanical debridement with a rigid bronchoscope, then placement of the endobronchial brachytherapy stent. Prior to each brachytherapy session, the patient tolerated the placement of the afterloading catheter via flexible bronchoscopy with no complications. The afterloading catheter remained in place with no movement during each brachytherapy session. The patient underwent three sessions of brachytherapy with no complications. The endobronchial brachytherapy stent was left in place after the completion of all of the brachytherapy treatment as the patient benefited from the improved airway patency provided by the stent. Flexible bronchoscopy showed dramatically decreased tumor burden with each successive brachytherapy session. The surrounding normal healthy endobronchial tissue was unaffected by the high-dose radiation received during the brachytherapy sessions. There was no stent migration seen via flexible bronchoscopy. References • Villanueva AG, Lo TC, Beamis JF Jr. Endobronchial brachytherapy. Clinics in Chest Medicine. 16(3): 445-54, 1995. • Colt HG, Dumon JF: Airway Stents. Present and future. Clinics in Chest Medicine. 16(3): 465-78, 1995. • Unger M. Endobronchial therapy of neoplasms. Chest Surgery Clinics of North America. 13(1): 129-47, 2003. • Gejerman G, Mullokandov EA, Bagiella E, et al. Endobronchial brachytherapy and external-beam radiotherapy in patients with endobronchial obstruction and extrabronchial extension. Brachytherapy. 1(4): 204-10, 2002. • Duhamel DR, Harrell JH. Laser bronchoscopy. Chest Surgery Clinics of North America. 11(4): 769-89, 2001. • Langendijk H, de Jong J, Tjwa M, et al. External irradiation versus external irradiation plus endobronchial brachytherapy in inoperable non-small cell lung cancer: a prospective randomized study. Radiotherapy & Oncology. 58(3): 257-68, 2001. • Petera J, Neumanova R, Vrba M, et al. HDR intraluminal brachytherapy in the treatment of malignant bronchial obstructions. Neoplasma. 47(1): 56-9, 2000. • Quantrill SJ, Burt PA, Barber PV, et al. Treatment of endobronchial metastases with intraluminal radiotherapy. Respiratory Medicine. 94(4): 369-72, 2000. • Marsiglia H, Baldeyrou P, Lartigau E, et al. High-dose-rate brachytherapy as sole modality for early-stage endobronchial carcinoma. International Journal of Radiation Oncology, Biology, Physics. 47(3): 665-72, 2000. • Stephens KE Jr, Wood DE. Bronchoscopic management of central airway obstruction. Journal of Thoracic & Cardiovascular Surgery. 119(2): 289-96, 2000. • Sheski FD, Mathur PN. Cryotherapy, electrocautery, and brachytherapy. Clinics in Chest Medicine. 20(1): 123-38, 1999. • Johnston MR, Grondin S. The role of endoscopy in the staging and management of lung metastases. Chest Surgery Clinics of North America. 8(1): 49-58, 1998. • Ofiara L, Roman T, Schwartzman K. Local determinants of response to endobronchial high-dose rate brachytherapy in bronchogenic carcinoma. Chest. 112(4): 946-53, 1997. • Bowman RV. Recent advances in managing non-small-cell lung cancer: Endobronchial palliative therapy. Medical Journal of Australia. 166 Suppl: S17-20, 1997. For five columns, line up guides with these boxes