Download
1 / 1
50 likes | 445 Views
The whole tissue: The whole tissue V30 was significantly reduced for VMAT-1 compared with VMAT-2 and IMRT, although the whole tissue V50 and V70 were similar for all treatment techniques. On the other hand, the whole tissue V10 was the most significantly reduced for IMRT (Table 2, Fig. 5).

E N D
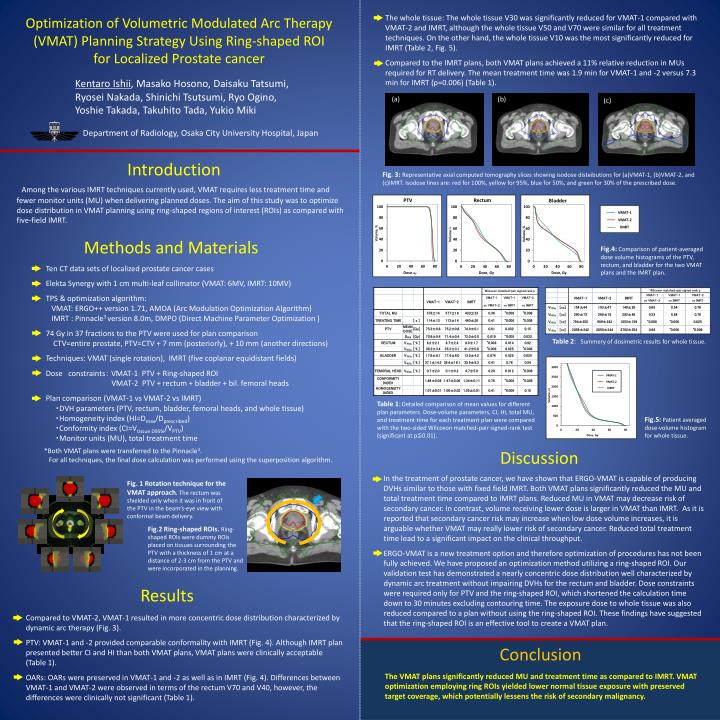
The whole tissue: The whole tissue V30 was significantly reduced for VMAT-1 compared with VMAT-2 and IMRT, although the whole tissue V50 and V70 were similar for all treatment techniques. On the other hand, the whole tissue V10 was the most significantly reduced for IMRT(Table 2,Fig.5). Compared to the IMRT plans, both VMAT plans achieved a 11% relative reduction in MUs required for RT delivery. The mean treatment time was 1.9 min for VMAT-1 and -2 versus 7.3 min for IMRT (p=0.006)(Table1). OptimizationofVolumetricModulatedArcTherapy(VMAT)PlanningStrategyUsingRing-shapedROI forLocalizedProstatecancer VMAT-1 KentaroIshii, MasakoHosono, DaisakuTatsumi, RyoseiNakada,Shinichi Tsutsumi, Ryo Ogino,YoshieTakada, Takuhito Tada,YukioMiki VMAT-2 VMAT-1 VMAT-2 IMRT IMRT (a) (b) (c) Department of Radiology, Osaka City University Hospital, Japan Introduction Fig. 3:Representativeaxialcomputedtomographyslicesshowingisodosedisteibutionsfor(a)VMAT-1,(b)VMAT-2,and (c)IMRT.Isodoselinesare:redfor100%,yellowfor95%,bluefor50%,andgreenfor30%oftheprescribeddose. Among the various IMRT techniques currently used, VMAT requires less treatment time and fewer monitor units (MU) when delivering planned doses. The aim of this study was to optimize dose distribution in VMAT planning using ring-shaped regions of interest (ROIs) as compared with five-fieldIMRT. PTV Rectum Bladder Volume, % Volume, % Volume, % MethodsandMaterials Fig.4:Comparisonofpatient-averaged dosevolumehistogramsofthePTV,rectum,andbladderforthetwoVMATplansandtheIMRTplan. Ten CTdata sets of localized prostate cancer cases Elekta Synergy with 1 cm multi-leaf collimator(VMAT:6MV,IMRT:10MV) TPS&optimizationalgorithm: VMAT:ERGO++version1.71,AMOA(ArcModulationOptimizationAlgorithm) IMRT:Pinnacle3 version 8.0m,DMPO(Direct Machine Parameter Optimization ) 74 Gy in 37 fractions to the PTV were used for plan comparison CTV=entire prostate,PTV=CTV +7mm(posteriorly),+10mm(anotherdirections) Techniques:VMAT (singlerotation),IMRT(fivecoplanarequidistantfields) Doseconstraints: VMAT-1PTV+Ring-shapedROI VMAT-2PTV+rectum+bladder+bil.femoralheads Plancomparison(VMAT-1vsVMAT-2vsIMRT) ・DVHparameters(PTV,rectum,bladder,femoralheads,andwholetissue) ・Homogeneity index (HI=Dmax/Dprescribed) ・Conformity index (CI=Vtissue D95%/VPTV) ・Monitor units (MU), total treatment time Dose, Gy Dose, Gy Dose, Gy Table2:Summeryofdosimetricresultsforwholetissue. Volume, cc Table1:Detailedcomparisonofmeanvaluesfordifferentplanparameters.Dose-volume parameters, CI, HI, totalMU, and treatment time for each treatment plan were compared with the two-sided Wilcoxon matched-pair signed-rank test(significantatp≦0.01). Fig.5:Patient averaged dose-volume histogram forwholetissue. Dose, Gy *Both VMAT plans were transferred to the Pinnacle3. For all techniques, the final dose calculation was performed using the superposition algorithm. Discussion In the treatment of prostate cancer, we have shown that ERGO-VMAT is capable of producing DVHs similar to those with fixed field IMRT. Both VMAT plans significantly reduced the MU and total treatment time compared to IMRT plans. Reduced MU in VMAT may decrease risk of secondary cancer. Incontrast, volume receiving lower dose is largerinVMATthanIMRT. Asit is reported that secondary cancer risk may increase when low dose volume increases, it is arguable whether VMAT may reallylower risk of secondary cancer. Reduced total treatment time lead to a significantimpact on theclinical throughput. ERGO-VMAT is a new treatment option and therefore optimization of procedures has not been fully achieved. We have proposed an optimization method utilizing a ring-shaped ROI. Our validation test has demonstrated a nearly concentric dose distribution well characterized by dynamic arc treatment without impairing DVHs for therectum and bladder. Dose constraints were required only for PTV and the ring-shaped ROI,whichshortenedthe calculation time down to 30 minutes excluding contouring time. The exposure doseto whole tissue was also reduced compared to a plan without using the ring-shaped ROI. These findings have suggested that the ring-shaped ROI is an effective toolto create a VMAT plan. Fig. 1RotationtechniquefortheVMATapproach.The rectum was shielded only when it was in front of the PTV in the beam’s-eye view with conformal beam delivery. Fig.2 Ring-shaped ROIs.Ring-shaped ROIs were dummyROIsplaced on tissues surrounding the PTV with a thickness of 1 cm at a distance of 2-3 cm from the PTV and were incorporated in the planning. Results Compared to VMAT-2, VMAT-1 resulted in more concentric dose distribution characterized by dynamic arc therapy(Fig. 3). PTV: VMAT-1 and -2 provided comparable conformality with IMRT(Fig. 4). Although IMRT plan presented better CI and HI than both VMAT plans, VMAT plans were clinically acceptable(Table1). OARs: OARs were preserved in VMAT-1 and -2 as well as in IMRT(Fig. 4). Differences between VMAT-1 and VMAT-2 were observed in terms of the rectum V70 and V40, however, the differences were clinically notsignificant(Table1). Conclusion The VMAT plans significantly reduced MU and treatment time as compared to IMRT. VMAT optimization employing ring ROIs yielded lower normal tissue exposure with preserved target coverage, which potentially lessens the risk ofsecondary malignancy.