Download
1 / 42
440 likes | 586 Views
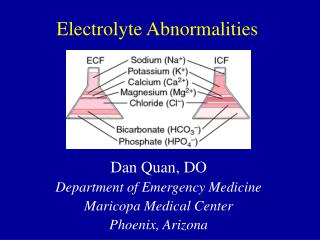
ELECTROLYTE DISASTERS. POTASSIUM. JOSE-MARIE EL-AMM NEPHROLOGY DIVISION WSU/DMC/HUH AUGUST, 2006. COMPOSITION OF BODY FLUID COMPARTMENTS. COMPOSITION OF ECF AND ICF ECF ICF Na 141 10 K 4.1 120-150 Cl 113 3 HCO 3 26 10 PHOSPHATE 2.0 140 (ORGANIC). GENERATION OF THE RMP.

E N D
ELECTROLYTE DISASTERS POTASSIUM JOSE-MARIE EL-AMM NEPHROLOGY DIVISION WSU/DMC/HUH AUGUST, 2006
COMPOSITION OF BODY FLUID COMPARTMENTS COMPOSITION OF ECF AND ICF ECF ICF Na14110 K 4.1120-150 Cl 113 3 HCO3 26 10 PHOSPHATE2.0140(ORGANIC)
VIRTUALLY ALL K EXCRETION OCCURS IN THE CCD MAJOR SITE OF K+ SECRETION Mid to Late DT and CCD 70-80% 600-700 mmol 15-20% 3000 mmol 60-90 mmol
Collecting tubules have selective Na channels in luminal surface (favored movement by Na levels low in cells and intracellular negativity). Pumped out of tubular cells by NaK-ATPase. Tubular lumen negatively charged and favors K movement into lumen by K channels. Aldo when combined with its receptor enhances Na reabsorption & K secretion via # Na channels & # NaK-ATPase pumps. Amiloride & Triamterene close Na channels directly Spironolactone competes w/ aldosterone ANP inhibits Na reabsorption by closing Na channels
HYPERKALEMIA • PSEUDOHYPERKALEMIA • SHIFTS • IMPAIRED RENAL EXCRETION
PSEUDOHYPERKALEMIA • MECHANICAL TRAUMA • INCREASED WBC • INCREASED PLATELETS
A 30 YEAR OLD MAN WITH TYPE 1 DIABETES MELLITUS IS COMATOSE. EXAM: BP 110/70 HR 100/MIN LYING 80/50 116 AT 45 ° TEMP 101 ° RR 24 LABS 128 94 34 538 6.1 11 1.9 WHY IS HIS POTASSIUM HIGH? !!!!! INTAKE/SHIFT/OUTPUT !!!!!
A 30 YEAR OLD MAN WITH TYPE 1 DIABETES MELLITUS IS COMATOSE. • Low serum sodium • Corrected Na= 128 + 7 = 135 • Low bicarbonate • <14 so metabolic acidosis AG= 23 • Corrected bicarb 24 • Elevated BUN/creatinine • ARF vs. CRF vs. Acute on Chronic • Hyperkalemia
HORMONES THAT SHIFT K INTO CELLS ACTIVATED BY 2ADRENERGICS 3 Na+ 2 K+ ELECTROGENIC ATP ADP Na+ K+ GLUCOSE ATP H+ ACTIVATED BY INSULIN ADP ACTIVATED BY INSULIN ELECTRONEUTRAL SYNTHESIS OF NEW NaK ATPase G6P2- (CREATES NEW ANIONS)
BUFFERING OF H+ AND THE K+ SHIFT H+ HYPOXIA, NO INSULIN HCl Cl- L-LACTATE -, -HB - H+ L-LACTATE -, -HB - H+ H-BUFFER+ H-BUFFER+ BUFFER BUFFER K SHIFTS OUT OF CELL IN ACIDOSIS WITH HCl-NOT ORGANIC ACIDOSIS K+ K EXCRETION ALTERED BY ALDOSTERONE, RENAL STATUS KIDNEY
SHIFTS • Rhabdomyolysis; tissue breakdown • Drugs; Digoxin, succinyl choline • DKA, hyperosmolar state
54 YEAR OLD MAN WITH MILD RENAL FAILURE. C/O DIFFICULTY IN GETTING OUT OF CHAIRS. HE RECENTLY WAS STARTED ON A LOW SODIUM DIET BUT NO NEW MEDICATIONS. EXAM: SLIGHTLY DECREASED SKIN TURGOR MARKED PROXIMAL MUSCLE WEAKNESS LABS: ECG HAS PEAKED T WAVES, WIDENED QRS 130 98 pH=7.32 9.8 17 CREATININE 2.7 (WAS 2.1) “mild hemolysis” THE INTERN DRAWS BLOOD TO REPEAT THE LABS (R/O “LAB ERROR”). THE RESIDENT HAS A SEIZURE.WHY?
LABORATORY ERROR IS NOT ASSOCIATED WITH SYMPTOMS! THIS MAN HAS BOTH SKELETAL MUSCLE AND CARDIAC MUSCLE SYMPTOMS OF HYPERKALEMIA. WHY DID HE SUDDENLY BECOME HYPERKALEMIC? WHY IS HIS POTASSIUM HIGH? !!!!! INTAKE/SHIFT/OUTPUT !!!!!
IS HE TAKING A SALT SUBSTITUTE???? CRF: RENAL DISEASE CONTRIBUTES BUT DIDN’T CAUSE HIS K PROBLEMS. PEOPLE WITH CRF CAN HAVE TROUBLE WITH SODIUM CONSERVATION IF THERE ARE SUDDEN CHANGES IN THEIR INTAKE. DECREASED TOTAL BODY SODIUM LEADS TO DECREASED RENAL BLOOD FLOW, DECREASED Na PAST THE DISTAL TUBULE AND HENCE DECREASED K EXCRETION. !!!!! INTAKE/SHIFT/OUTPUT !!!!!
FACTORS THAT DECREASE URINARY POTASSIUM EXCRETION 1.LOW URINE FLOW RATES 2.DECREASED Na DELIVERY TO DISTAL TUBULE (ARF, AGN, ESLD) 3.DECREASED MINERALOCORTICOID ACTIVITY (Renin-Ag system)
VIRTUALLY ALL K EXCRETION OCCURS IN THE CCD MAJOR SITE OF K+ SECRETION K+ H+ ALDO Na+ NONALDO Na+ K+ H2O + CO2 H2CO3 HCO3+ +H+
TREATMENT OF HYPERKALEMIA 1.CALCIUM10mL OF 10% Ca GLUCONATE OVER 10 MINUTES 2.INSULIN10 U IVP (REGULAR) WITH 50mL 50% DEXTROSE 3.ALBUTEROL10 mg NEBULIZED 0.5 mg IV 4.KAYEXALATE30-60 G PO OR 60 G AS ENEMA 5.HEMODIALYSIS
TREATMENT OF HYPERKALEMIA 1.CALCIUM 10mL OF 10% Ca GLUCONATE OVER 10 MINUTES 2.INSULIN10 U IVP (REGULAR) WITH 50mL 50% DEXTROSE 3.ALBUTEROL10 mg NEBULIZED 0.5 mg IV 4.KAYEXALATE30-60 G PO OR 60 G AS ENEMA 5.HEMODIALYSIS
A 22 YEAR OLD COMPLAINS OF FATIGABILITY AND WEAKNESS. PHYSICAL EXAM: BP 122/68 HR 72/MIN NO ORTHOSTATIC CHANGES NO EDEMA LABS: 135 85 2.1 45 UNa=80 UK=70 WHAT TEST(S) WILL HELP YOU MAKE THE DIAGNOSIS? WHY IS HIS POTASSIUM LOW? !!!!! INTAKE/SHIFT/OUTPUT !!!!!
METABOLIC ALKALOSIS AND HYPOKALEMIA 1. VOMITING 2. DIURETIC USE 3. BARTTER’S/GITELMAN’S THE LACK OF HYPERTENSION RULES OUT MINERALOCORTICOID OR MINERALOCORTICOID-LIKE EXCESS HORMONES
LABS: 135 85 UNa=80 UK=70 2.1 45 URINE CHLORIDE = 6 DIAGNOSIS IS VOMITING WITH URINARY K LOSSES FROM THE OSMOTIC DIURESIS AND SECONDARY HYPERALDOSTERONISM URINE CHLORIDE = 60 DIAGNOSIS IS RECENT USE OF DIURETICS OR BARTTER’S SYNDROME (or GITELMAN’S SYNDROME)
FACTORS THAT INCREASE URINARY POTASSIUM LOSSES 1. HIGH URINE FLOW RATES 2. INCREASED Na DELIVERY TO DISTAL TUBULE 3. INCREASED MINERALOCORTICOID ACTIVITY 4. ALKALOSIS 5. POORLY REABSORBED LUMINAL ANION
VIRTUALLY ALL K EXCRETION OCCURS IN THE CCD MAJOR SITE OF K+ SECRETION 480 mmol 60-90 mmol 720 mmol 3000 mmol 60 mmol
TREATMENT OF HYPOKALEMIA • The safest route of replacement is PO. • KCl is the preparation of choice for K w/ • ECF volume contraction, • diuretic use • metabolic alkalosis. • Potassium bicarbonate (or citrate) for K w/ • RTA • diarrhea associated K losses. • K phosphate for K w/ • anabolism (TPN) • phosphate depletion (recovering DKA).
TREATMENT OF HYPOKALEMIA • The goal of emergency therapy should be to get the patient out of danger rapidly but replacing the entire potassium deficit quickly is not desirable. • During chronic hypokalemia, renal mechanisms develop to minimize aldosterone-induced K losses. These may persist for 1 to 2 days after correction. • Aggressive, rapid replacement of potassium may lead to hyperkalemia
TREATMENT OF HYPOKALEMIA • Peripheral IV potassium infusions should be less than 60mEq/L to avoid vascular spasm or sclerosis. • Rates should be less than 20mEq/hr unless done in a monitored setting. • 20mEq of KCl in 1 liter of D5W can lead to a further drop in serum potassium. • Concentrated potassium solutions through a central line can lead to dangerous cardiac sequelae.
A 54 YEAR OLD MAN WITH NO PRIOR MEDICAL HISTORY COMPLAINS OF CHRONIC FATIGUE. EXAM: BP 100/60 WITHOUT ORTHOSTATIC CHANGE. NO EDEMA LABS: 137 106 28 UNa=50 90 UK=48 6.8 20 1.0 Uosm=450 !!!!! INTAKE/SHIFT/OUTPUT !!!!!
TTKG: TRANSTUBULAR POTASSIUM GRADIENT ASSUME A TTKG OF 3.3 10 mmol/L 10 mmol/L 3 mmol/L K+ CORTEX 300 mOsm/L CCD OSM=300 1 LITER LEAVES CCD OSM MEDULLA 0.75 L 0 L MCD 0.25 L=40mmol/L UOSM=1200 1 L=10mmol/L UOSM=300 URINE
TTKG TTKG= [ K+ ]urine /(urine/plasma)osm / [ K+ ]plasma ASSUMPTIONS: 1. OSMOLALITY IS KNOWN IN CCD. TTKG CANNOT BE USED IF UOSM< POSM 2. WATER REABSORPTION IN MCD CAN BE ESTIMATED, BUT IF ANP IS COMPLETELY SHUT OFF THERE IS Na REABSORPTION IN THE MCD AND TTKG IS AN OVERESTIMATE. 3.K+ IS NOT REABSORBED OR SECRETED IN MCD. THIS IS TRUE UNLESS PROFOUND K DEPLETION OR TAKING “INDUSTRIAL” DOSES OF K 4. THE K IN PLASMA REFLECTS THE PERITUBULAR K
A 54 YEAR OLD MAN WITH NO PRIOR MEDICAL HISTORY COMPLAINS OF CHRONIC FATIGUE. EXAM: BP 100/60 WITHOUT ORTHOSTATIC CHANGE. NO EDEMA LABS: 137 106 28 UNa=50 90 UK=48 6.8 20 1.0 Uosm=450
137 106 28 UNa=50 90 UK=48 6.8 20 1.0 Uosm=450 TTKG={48 (450 289)} 6.8= 4.5 HYPERKALEMIA STIMULATES ALDOSTERONE RELEASE. IN HYPERKALEMIA THE TTKG SHOULD BE 10 OR ABOVE. THIS FELLOW LACKS SUFFICIENT MINERALOCORTICOID ACTIVITY.
ADDISON’S DISEASE A LACK OF ALDOSTERONE LEADS TO: INCREASED URINARY SODIUM LOSSES HYPERKALEMIA METABOLIC ACIDOSIS