Download
1 / 12
120 likes | 135 Views
This case study details the management of George, a 9-year-old West Highland White Terrier presenting with PU/PD, vomiting, and collapse. Clinical findings, diagnostic workup, treatment, and considerations are discussed, highlighting the challenges in managing severe hyperglycemia and related complications.

E N D
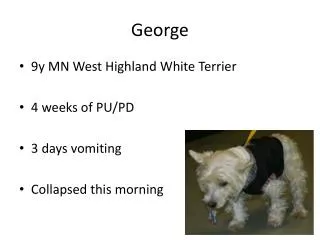
George • 9y MN West Highland White Terrier • 4 weeks of PU/PD • 3 days vomiting • Collapsed this morning
Physical examination • Stuporous • Cardiovascular examination • HR 150 bpm • Bounding pulses • Pink mucous membranes • No abdominal distension/pain
George • PCV/TS 58%/80g/l • Ketonaemic • BUN 15mmol/l • Creatinine 180µmol/l • Glucose 25mmol/l
George - Electrolytes and blood gas • K 3.5mmol/l • pH 7.2mmol/l
George – Problem list • Dehydration • Severe hyperglycaemia • Azotaemia • Hypokalaemia • Metabolic acidosis
George • Considerations • Inappropriate insulin storage/handling/admin • Inappropriate dosage • Concurrent disease • Urinary tract infection (sediment exam + urine culture) • Pancreatitis (u/s + cPLI) • Hyperadrenocorticism • Other
George - diagnostics • Urinalysis • Glucosuric (4+) • Ketonuric (3+) • WBCs on sediment examination • Abdominal ultrasound • Unilateral pyelectasia
George • Moderate hypovolaemia • Dehydration • Hypokalaemia • ? Fluid plan
George • Correct hypovolaemia first Bolus crystalloid 20ml/kg over 20 minutes Improvement in clinical signs • On going fluid plan?
George • Started intravenous insulin protocol • Supplemented potassium after resuscitation • Supplemented phosphorus
George • Intravenous antibiosis whilst culture pending • Augmentin 20mg/kg q8h • Slowly improved over 48 hours • Started on s/c insulin protocol
George • George had pyelonephritis • George’s owner had withheld insulin whilst he was anorexic