Download
1 / 1
10 likes | 63 Views
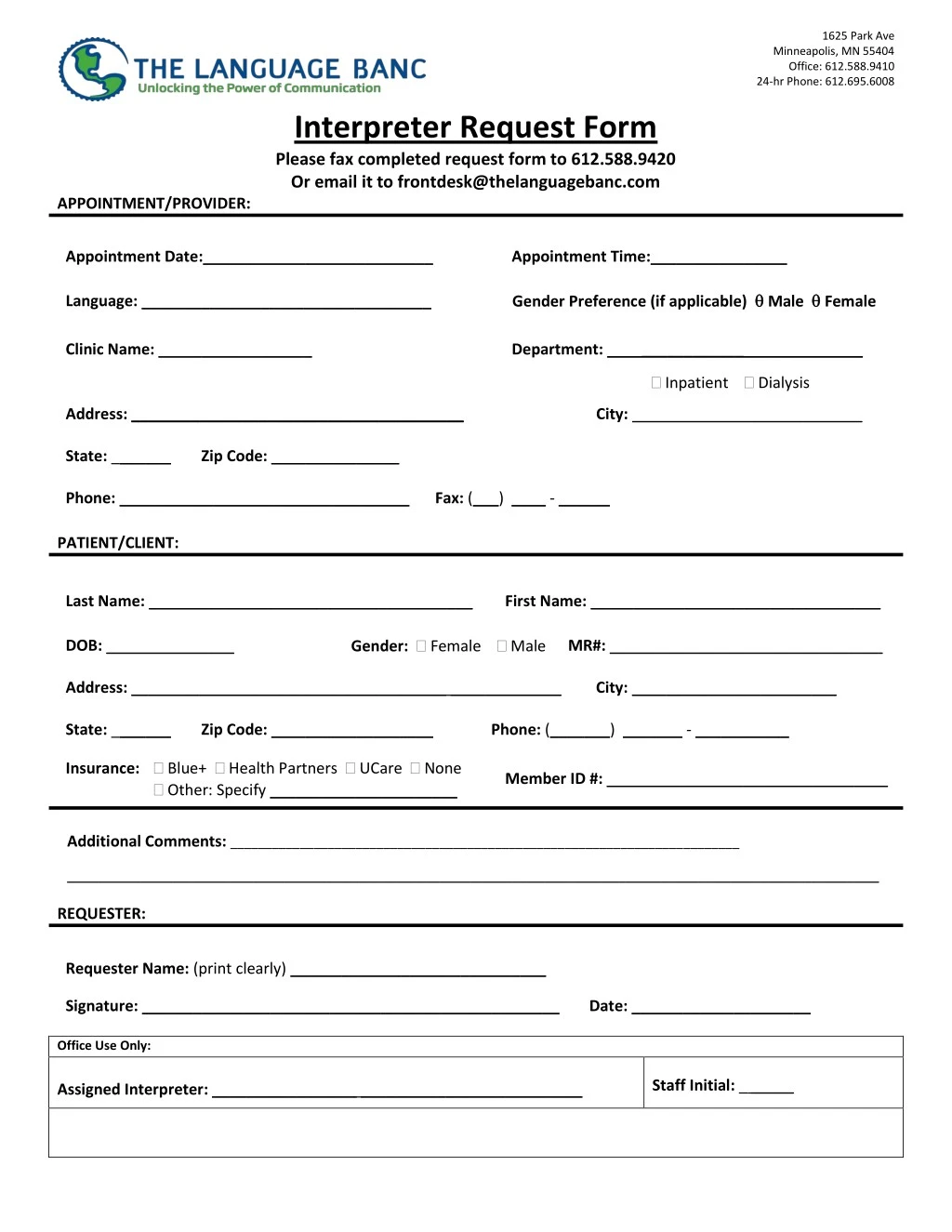
To obtain an Interpreter, please complete the appropriate Interpreter Request Form with as much notice as possible. The Language Banc provides language interpreters to courts, hospitals, clinics and healthcare providers throughout the Minneapolis, MN and surrounding cities. Visit here: https://www.thelanguagebanc.com/<br>

E N D
1625 Park Ave Minneapolis, MN 55404 Office: 612.588.9410 24-hr Phone: 612.695.6008 Interpreter Request Form Please fax completed request form to 612.588.9420 Or email it to frontdesk@thelanguagebanc.com APPOINTMENT/PROVIDER: Appointment Date:___________________________ Appointment Time:________________ Gender Preference (if applicable) Male Female Language: __________________________________ Clinic Name: __________________ Department: ______________________________ Inpatient Dialysis Address:_______________________________________ City: ___________________________ State: _______ Zip Code: _______________ Phone: __________________________________ Fax: (___) ____ - ______ PATIENT/CLIENT: Last Name: ______________________________________ First Name: __________________________________ Gender: Female Male DOB: _______________ MR#: ________________________________ Address: _____________________________________ _____________ City: ________________________ State: _______ Zip Code: ___________________ Phone: (_______) _______ - ___________ Insurance: Blue+ Health Partners UCare None Other: Specify ______________________ Member ID #: _________________________________ Additional Comments:_________________________________________________________________________ ___________________________________________________________________________________________________________________________________ REQUESTER: Requester Name: (print clearly) ______________________________ Signature: _________________________________________________ Date: _____________________ Office Use Only: Assigned Interpreter: _________________ __________________________ Staff Initial: _ _____