Download

1 / 20
411 likes | 787 Views
Initial Combination Treatment in Hypertension: Who Are the Candidates. George Bakris, MD, F.A.S.H., F.A.S.N. Professor of Medicine Director, Hypertensive Disease Unit University of Chicago, Pritzker School of Medicine Chicago, IL . 50% response. Patients With Response* (%).

E N D
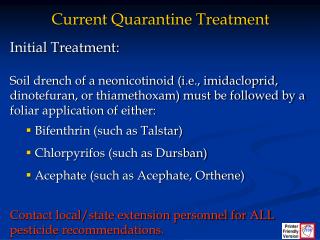
Initial Combination Treatment in Hypertension: Who Are the Candidates George Bakris, MD, F.A.S.H., F.A.S.N. Professor of Medicine Director, Hypertensive Disease Unit University of Chicago, Pritzker School of Medicine Chicago, IL
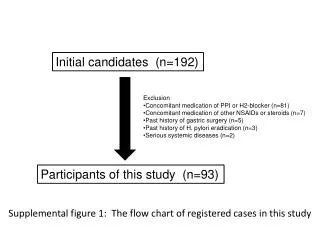
50% response Patients With Response* (%) α2 Agonist (clonidine) ACEI(captopril) α1 Antagonist(prazosin) CCB(dilitiazem) β-blocker(atenolol) Placebo Diuretic(HCTZ) Monotherapy for Hypertension Is Inadequate in ~40% to 50% of Patients *Response = DBP <90 mm Hg at the end of titration period and having maintained a DBP of <95 mm Hg for 1 year without drug tolerance.Mean baseline BP = 152/99 mm Hg. Adapted from Materson BJ et al. Am J Hypertens. 1995;6:189-192.
Rationale for Fixed-Dose Combination Therapy: Background • Traditional antihypertensive therapy yields goal BP in <60% of treated hypertensive patients1-3 • Switching from one monotherapy to another is effective in only about 50% of patients1 • Most patients will require at least two drugs to attain goal BP (<140/90 mm Hg, or <130/80 mm Hg for patients with diabetes or chronic renal disease)4-6 BP = blood pressure Materson BJ et al. J Hum Hypertens. 1995;9(10):791-796. Messerli FH. J Hum Hypertens. 1992;6 Suppl. 2:S19-S21. Ram CV. J Clin Hypertens (Greenwich). 2004;6(10):569-577. Chobanian AV, et al. JAMA. 2003;289(19):2560-2572. Guidelines Committee. J Hypertens. 2003;21:1011-1053. American Diabetes Association. Diabetes Care. 2002;25(Suppl.1):S71-S73.
Growth of Fixed-Dose Combinations Monotherapy 87.6% 88.0% 88.6% 89.3% Fixed-Dose Combination 11.4% 12.4% 12.0% 10.7% IMS National Prescription Audit (NPA)
Ratio of Observed to Expected Incremental BP-Lowering Effects of Adding a Drug or Doubling the Dose According to Drug Class Adding a drug from another class (on average standard doses) Doubling dose of same drug (from standard dose to twice standard) 1.40 1.20 1.00 0.80 1.16 1.01 1.04 Incremental SBP reduction ratio of observed to expected additive effects 1.00 0.60 0.89 0.40 0.20 0.37 0.22 0 0.2 0.23 0.19 Thiazide Calcium channel blocker ACE inhibitor All classes Beta blocker Wald DS et al. Am J Med. 2009;122:290-300.
Multiple Medications Are Required to Achieve BP Control in Clinical Trials 1 2 3 4 SBP achieved (mm Hg) Trial ACCOMPLISH 131 ALLHAT 138 HOT 138 ACCORD (intensive)* 119 ACCORD (standard)* 133 INVEST 133 IDNT 138 RENAAL 141 ABCD 132 UKPDS 144 MDRD 132 AASK 128 Hyper-tension Diabetes Kidneydisease SBP=systolic blood pressure. *Target blood pressure control groups in ACCORD defined as <120 mm Hg (intensive) and <140 mm Hg (standard). Updated from Bakris G et.al Am J Kidney Dis 2000. The ACCORD Study Group. N Engl J Med. 2010 Mar 14. [Epub ahead of print] No. of BP medications
1.0 Odds Ratio 0–1 2–3 4–7 8+ Adherence and Pill Burden Odds of Being Adherent to Both Lipid- and BP-Lowering Rx Number of Medications in Addition to Lipid- and BP-Lowering Rx Chapman RH et al. Circulation. 2003;108(17 suppl IV):IV-756-757.
Free Combination (ACEI+CCB) (n=3367) 69 Fixed-Dose Combination (ACEI/CCB) * (n=2839) 88 0 20 40 60 80 100 Medication Possession Ratio (MPR) Improved Adherence With Fixed-Dose Combination Therapy Compared With Free-Combination Therapy • Because this was a retrospective analysis of administrative claims data, patients were not randomly assigned and could not be matched by any empirical methods. Although we know the prescriptions were filled based on these claims data, it is unknown if patients specifically took the medication as prescribed. • Levels of disease severity as defined by clinical measurements were not available within the design of the study. • Analyses of concomitant drug classes were used to estimate disease severity, as polypharmacy may affect adherence. Other factors may exist that might have influenced selection or use of antihypertensive agents, which could not be captured or assessed in the study. *P<.0001.MPR = number of days of therapy for medication dispensed 365 days of study follow-up. Gerbino PP, Shoheiber O. Am J Health-Syst Pharm. 2007;64:1279-1283.
Compliance Gap Between Fixed-dose Combination and Dual Agent Regardless of Concomitant Medications US pharmacy claims data (n=6,206) *p=<0.0001 * * * * * Medication-possession ratio (MPR) * * Number of concomitant drugs Wanovich. Am J Hypertens 2004;17:223A
Risk Ratio(95% CI) Study % Weight Su WJ et al 0.89 (0.51,1.57) 0.6 Geiter LJ et al 0.88 (0.55,1.42) 1.1 Eron JJ et al 0.78 (0.55,1.11) 1.5 Taylor AA et al 0.74 (0.67,0.81) 25.3 Dezii CM et al 0.74 (0.65,0.84) 12.9 NDC Dataset 0.81 (0.77,0.86) 43.2 Dezii CM et al 0.71 (0.62,0.80) 11.7 Melikian C et al 0.50 (0.35,0.71) 3.1 Melikian C et al 0.47 (0.22,1.01) 0.6 Overall (95% CI) 0.76 (0.73,0.79) 0.1 1 10 Risk Ratio Adherence With Fixed-Dose Combinations Compared With Free-Drug Combinations Bangalore S et al. Am J Med. 2007;120:713-719.
Concomitant Use of Antihypertensive Drugs Diuretics AT1-receptorblockers -blockers Calciumantagonists -blockers ACE inhibitors Preferred Combinations Controversial Combinations Adapted from Mancia et al. 2007 ESH-ESC Practice Guidelines for the Management of Arterial Hypertension. J Hypertension 2007; 25(9): 1751-62
ACCOMPLISH: Design Free add-on antihypertensive agents* N = 11,462 with systolic hypertension and CV or renal disease or target organ damage Amlodipine 10 mg +benazepril 40 mg Amlodipine 5 mg +benazepril 40 mg Amlodipine 5 mg +benazepril 20 mg Screening Randomization Benazepril 20 mg + HCTZ 12.5 mg Benazepril 40 mg + HCTZ 12.5 mg Benazepril 40 mg + HCTZ 25 mg Titrated to achieve BP <140/90 mmHg or <130/80 mmHg with diabetes/renal insufficiency Free add-on antihypertensive agents* 14 Days Day 1 Month 1 Month 2 Month 3 Year 5 *Beta- or alpha- blockers, clonidine, loop diuretics Jamerson KA et al. Am J Hypertens. 2004;17:793-801; Presented at: ACC 2008 Chicago; ClinicalTrialResults.org.
ACCOMPLISH – Blood Pressure Results ACEI / HCTZ N=5733 CCB / ACEI N=5713 mm Hg 132.5 mmHg Difference of 0.9 mmHg p<0.001 131.6 mmHg Month 5757 5408 5222 5033 4825 4299 2529 1042 5740 5404 5178 5010 4866 4298 2804 1074 Patients DBP: 73.3 DBP: 74.4 Jamerson et al. NEJM. 2008; 359(23); 2417-2428.
ACCOMPLISH – Primary Endpoint 20% Risk Reduction ACEI / HCTZ 679 CCB / ACEI 552 Cumulative event rate p = 0 .0 0 1 Time to 1st CV morbidity/mortality (days) HR (95% CI): 0.80 (0.72, 0.90) Jamerson et al. NEJM. 2008; 359(23); 2417-2428.
STITCH: Objective and Study Design Objective: To assess if the use of a fixed-dose combination (FDC) as initial treatment of hypertension will improve the proportion of patients reaching goal BP as compared to the use of the Canadian Hypertension Education Program (CHEP) algorithm Design: 2104 patients from 45 Primary Care Practices in Southern Ontario Guideline-Care Algorithm (27 Practices) STITCH-Care Algorithm (18 Practices) Primary endpoint: Proportion of patients reaching BP target(practice-level) at 6 months Feldman RD et al. Hypertension. 2009;53:646-653.
STITCH: Study Design (cont’d) CHEP Guidelines:Treatment of hypertension withoutother compelling indications Target: SBP <140 DBP <90 mm Hg STITCH –Care Algorithm Initial therapy with a low dose ACE-diuretic or ARB/diuretic combination Lifestyle Modification Therapy BP controlled? Yes No Continue with current therapy Up-titrate combination therapy successively to the highest dose Thiazide Diuretic ACE-I ARB Long-acting CCB Beta-blocker Yes No Continue with current therapy Add calcium channel blocker and up-titrate Dual Combination Yes No Continue with current therapy Add alpha blocker, beta-blocker or spironolactone Triple or Quadruple Therapy Feldman RD et al. Hypertension. 2009;53:646-653.
STITCH: Main Results Feldman RD et al. Hypertension. 2009;53:646-653.
STITCH: Predictors of AchievingBP Target *The analysis was conducted using a modified Poisson regression model that evaluated patient-level data. †P values were derived by adjustment for clustering in the model. Feldman RD et al. Hypertension. 2009;53:646-653.
Conclusions • Monotherapy is the standard initial treatment for reducing BP, with stepwise increases in dose if the desired decrease in BP is not achieved • Combining drugs from different classes is approximately 5 times more effective in lowering BP than increasing the dose of 1 drug • Combination therapy is the preferred initial strategy in the treatment of high BP
DRUG COMBINATIONS IN HYPERTENSION: RECOMMENDATIONS *SPC available in the US Gradman AH et al. J Am Soc Hypertens 4:42-50, 2010.