Download
1 / 25
250 likes | 384 Views
Use of the Refractory Period in the Treatment of Exercise- Induced Bronchoconstictions in a Collegiate Football Player: A Case Study. Brian G Pietrosimone, M.Ed, ATC John MacKnight, MD Ethan Saliba, PhD, PT,ATC,SCS Jay Hertel, PhD, ATC. Asthma.

E N D
Use of the Refractory Period in the Treatment of Exercise- Induced Bronchoconstictions in a Collegiate Football Player: A Case Study Brian G Pietrosimone, M.Ed, ATC John MacKnight, MD Ethan Saliba, PhD, PT,ATC,SCS Jay Hertel, PhD, ATC
Asthma • Exercise triggers asthma in 50 -90% of known Asthmatics (Parsons et al., Freed et al.) • 10 % of non – asthmatics report symptoms of asthma during exercise (Parsons et al.) • Wheezing • Coughing • Tightness in chest • Inability to catch one’s breath • Increased mucus production
Pathogenesis of EIB • The pathogenesis behind exercise induced bronchospasm is not fully understood (Tan et al. & Chang- Yeung) • Different Theories • Dehydration of mucosal lining • Bronchial mucosal hyperemia
Dehydration of Mucosal Lining • Cold, dry air causes dehydration of the mucus membrane • Water loss causes an increase in osmotic pressure • Mast Cell degranulation leads to inflammatory mediator release (Parsons & Mastronarde, Tan, Maler)
Hyperemia • Re- warming in the lungs causes distal airways to increase blood flow • Increased hydrostatic pressure in bronchial vasculature • Increased airway edema (Parsons & Mastronarde, Tan, Maler)
History • Setting • ACC, NCAA Division 1 Football Program • Climate Zone 3 • Athlete Demographics • 18 year old • Male • Single • Caucasian • Height: 6’ 2’’ • Weight: 258 pounds • Position: Defensive Line • Hometown in Climate Zone 3
Past Asthma History • Health history form – Indicated past history of asthma • Exercise was a stimulus • No other health problems, or family problems • Prescribed prior to enrolling at the University • Albuterol MDI prn- short-acting bronchodilator • Salmeterol (Serevent) MDI - long-acting bronchodilator • Fluticasone propionate (Flovent) MDI- inhaled corticosteroid
Differential Diagnosis • Exercise Induced Bronchospasm • Extrinsic Asthma • Chronic Bronchitis • Cardiomyopathy
FEV1 • Spirometry measurements reported a decrease of 19% in FEV1 - confirming the diagnosis of EIB(Tan and Spector) • FEV1 = (Pretest FEV1 - Post test FEV1) x100 Pretest FEV1 • No significant findings on Echocardiogram
Pattern • Team Physician noticed pattern 2 h 4 h Real Time 6- 10 m 20-25 m 3h 3rd 4th 1st 2nd Game Time Unable to participate Refractory Period Able to participate
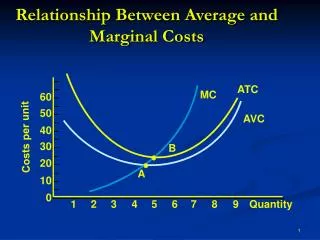
Refractory Period • The refractory period is the time in which the athlete remained asymptomatic after the first bout of symptoms • Refractory period occurs in 40% to 50% of asthmatics (Milgrom & Taussig )
Refractory Period • Theory suggests that a depletion in inflammatory mediators occurs with an initial bronchospasm (Freed & Chang- Yeung et al.) • Subsequent exercise results in no additional mediator release • The refractory period last for 2 to 4 hours after the first bout of EIA (Ben- Dov et al. & Wilson et al.)
Treatment • 75 minutes prior to game time under the supervision of the Team Physician • 4 x 50 yard sprints at a moderate intensity • Series of 5, 10 and 20 yard shuttle runs • 30 second rest was taken between each shuttle run in order to determine if the athlete had provoked sufficient bronchospasm to allow for a refractory period.
Treatment • Desired response was a bout of EIB large enough to provoke a subsequent refractory period • Athlete response • Wheezing • Coughing • Tightness in chest • Sputum production
Treatment • After team physician and athlete agreed that desired response had been reached: • Consciously slowed breathing rate • Albuterol (2 puffs) • 15-20 minute cool down time prior to team warm up
Treatment Effect 4.5 h 6-10 m 1.5 h 2.5 h 3.25- 3.5 h 75 min 3rd Onset of EIB Pre- game 1st 2nd 4th Able to play asthma free EIB Critical area: Ability for bronchospasms to return
Effectiveness of Treatment • Effectiveness was greatly reliant on the ability of physician and athlete to adequately induce the initial bronchospasm • During the Senior year • 72% of the games asthma free (8/11) • 2/3 bouts of EIB occurred in the second half • Rare additional Albuterol use with good effect
Uniqueness • The refractory period is a well documented phenomenon • It has not been documented as a treatment in the athletic population • This treatment worked consistently well and minimized the use of medication
Limitations with this Treatment • Time frame does not allow for treatment prior to practices • Many trials are needed to accurately predict refractoriness
Implications for Future Research • Can the refractory period be used routinely to effectively treat athletes? • Mechanisms behind the refractory period • Does the refractory period decrease EIB in athletes more effectively than medications?
What do I do with this Information? • Possible treatment strategy • Diagnosed athlete with breakthrough EIB • Rescue therapy in place • Provides comfort in return to play decisions for ATC and sports medicine team
Conclusion • The timing of the refractory period can be manipulated to coincide with the competition, preventing an exercise- induced bronchospasm during play.
References • 1. Parsons J, Mastronarde J. Exercise - induced bronchoconstriction in athletes. Chest. 2005;128:33966-33974. • 2. Freed A. Models and mechanisms of exerise-induced asthma. Eur Respir J. 1995;8:1770-1785. • 3. Tan R, Spector S. Exercise - Induced Asthma. Sports Med. 1998;25(1):1-6. • 4. Arif A, Delclos G, Lee E, Tortolero S, Whitehead L. Prevalence ad risk factors of asthma and wheezing among US adults: an analysis of the NHANES III data. Eur Respir J. 2003;21:827-833. • 5. Goodman D, Lozano P, Stukel T, Chang C, Hecht J. Has asthma medication use in children become more frequent, more appropriate, or both? Pediatrics. 1999;104:187-194. • 6. Ben-Dov I, Bar- Yishay E, Godfrey S. Refractory period after exercise induced asthma unexplained by respiratory heat loss. Am Rev Respir Dis. 1982;125:530- 534. • 7. Milgrom H, Taussig L. Keeping children with exercise- induced asthma active. Pediatrics. 1999;104:38-43. • 8. Chang- Yeung M, Vyas M, Grzybowski S. Exersice induced asthma. Am Rev Respir Dis. 1971(104):915 - 924. • 9. Mahler D. Exercised- induced asthma. Medicine and Science in Sports and Exercise. 1993;25:554-561. • 10. Haverkamp H, Dempsey J, Miller J. Repeat exercise normalizes the gas- exchange impairment induced by a previous exercise bout in asthmatic subjects. J Appl Physiol. 2005;99:1843- 1852. • 11. Anderson S, Daviskas E. The mechanism of exercise- induced asthma is. Allergy Clin Immunol. 2000;106:453-459. • 12. McFadden E, Nelson J, Skowronski M, Lenner K. Thermally induced asthma and airway drying. Am J Respir Crit Care Med. 1999;160:221-226. • 13. Wilson B, Bar-Or O, Seed L. Effects of humid air breathing during arm or treadmill exercise on exercise - induced bronchoconstriction and refractoriness. Am Rev Respir Dis. 1990(142):349- 352. • 14. Edmunds A, Tooley M, Godfrey S. Refractory period after exercise induced asthma: Its duration and relation to the severity of exercise. Am Rev Respir Dis. 1978;177:247- 255. • 15. Rosenthal R, Laube B, Hood D, Norman P. Analysis of refractory period after exercise and eucapnic voluntary hyperventilation challenge. Am Rev Respir Dis. 1990;141:368- 372. • 16. Matsumoto L, Araki H, Tsuda K, et al. Effects of swimming training on aerobic capacity and exercise induced brochoconstriction in children with bronchial asthma. Thorax. 1999;54:196-201.