Download
1 / 1
10 likes | 198 Views
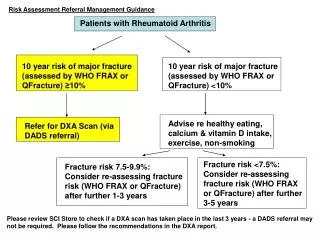
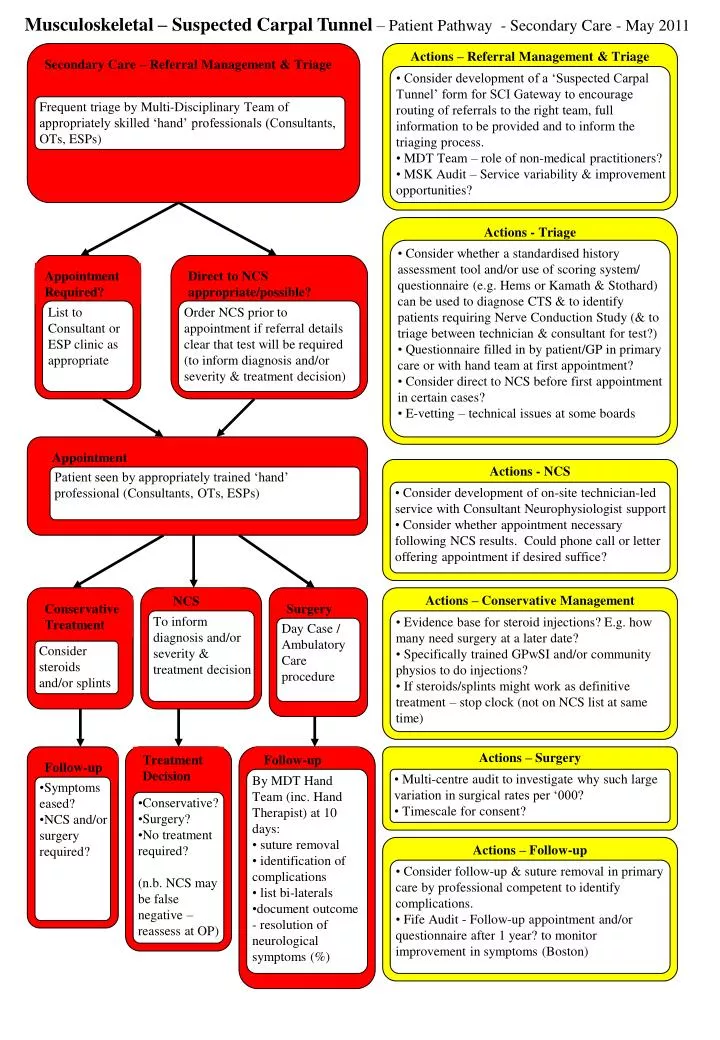
Musculoskeletal – Suspected Carpal Tunnel – Patient Pathway - Secondary Care - May 2011. Actions – Referral Management & Triage. Secondary Care – Referral Management & Triage.

E N D
Musculoskeletal – Suspected Carpal Tunnel – Patient Pathway - Secondary Care - May 2011 Actions – Referral Management & Triage Secondary Care – Referral Management & Triage • Consider development of a ‘Suspected Carpal Tunnel’ form for SCI Gateway to encourage routing of referrals to the right team, full information to be provided and to inform the triaging process. • MDT Team – role of non-medical practitioners? • MSK Audit – Service variability & improvement opportunities? Frequent triage by Multi-Disciplinary Team of appropriately skilled ‘hand’ professionals (Consultants, OTs, ESPs) Actions - Triage • Consider whether a standardised history assessment tool and/or use of scoring system/ questionnaire (e.g. Hems or Kamath & Stothard) can be used to diagnose CTS & to identify patients requiring Nerve Conduction Study (& to triage between technician & consultant for test?) • Questionnaire filled in by patient/GP in primary care or with hand team at first appointment? • Consider direct to NCS before first appointment in certain cases? • E-vetting – technical issues at some boards Appointment Required? Direct to NCS appropriate/possible? List to Consultant or ESP clinic as appropriate Order NCS prior to appointment if referral details clear that test will be required (to inform diagnosis and/or severity & treatment decision) Appointment Actions - NCS Patient seen by appropriately trained ‘hand’ professional (Consultants, OTs, ESPs) • Consider development of on-site technician-led service with Consultant Neurophysiologist support • Consider whether appointment necessary following NCS results. Could phone call or letter offering appointment if desired suffice? NCS Actions – Conservative Management Conservative Treatment Surgery To inform diagnosis and/or severity & treatment decision • Evidence base for steroid injections? E.g. how many need surgery at a later date? • Specifically trained GPwSI and/or community physios to do injections? • If steroids/splints might work as definitive treatment – stop clock (not on NCS list at same time) Day Case / Ambulatory Care procedure Consider steroids and/or splints Treatment Decision Follow-up Actions – Surgery Follow-up • By MDT Hand Team (inc. Hand Therapist) at 10 days: • suture removal • identification of complications • list bi-laterals • document outcome - resolution of neurological symptoms (%) • Multi-centre audit to investigate why such large variation in surgical rates per ‘000? • Timescale for consent? • Symptoms eased? • NCS and/or surgery required? • Conservative? • Surgery? • No treatment required? • (n.b. NCS may be false negative – reassess at OP) Actions – Follow-up • Consider follow-up & suture removal in primary care by professional competent to identify complications. • Fife Audit - Follow-up appointment and/or questionnaire after 1 year? to monitor improvement in symptoms (Boston)