Download
1 / 43
620 likes | 1.37k Views
Milk intolerance in infants. Food intolerance or food allergy ? Intolerance is not immune mediated For cow’s milk = lactose intolerant Lactose intolerance in infants = enteropathy Allergy is immune mediated IgE-mediated - local or systemic Non-IgE-mediated - local or systemic.

E N D
Milk intolerance in infants • Food intolerance or food allergy ? • Intolerance is not immune mediated • For cow’s milk = lactose intolerant • Lactose intolerance in infants = enteropathy • Allergy is immune mediated • IgE-mediated - local or systemic • Non-IgE-mediated - local or systemic
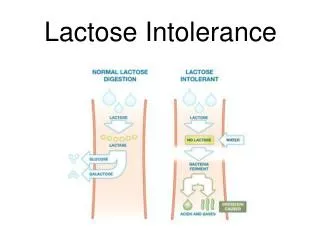
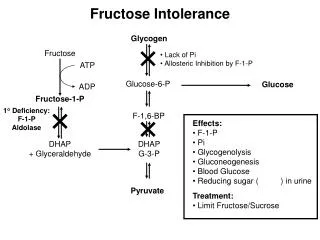
Lactose intolerance • Normal in most adults in the world • Tolerance mutation arose since dairy farming • North Europeans usually tolerant as adults • Lactase downregulated in teens • Always abnormal in infants • Very rare - congenital absence (Lapps) • Very common - enteropathy • Temporary – following rotavirus etc • Persistent – with mucosal allergic sensitisation
Eczema,GI symptoms T cells RespiratoryGI symptoms Eosinophils Urticaria,anaphylaxis Mast cells David Hill et al
Types of milk allergy • IgE-mediated – rapid onset • Systemic – anaphylaxis response • Localised to gut – secretion, dysmotility • Non-IgE-mediated – slow onset • Systemic – Eczema, asthma • Localised to gut – Enteropathy, colitis, eosinophilic GI disorders • Mixed IgE and Non-IgE-mediated
Detection of IgE-mediated food allergy usually straightforward • Usually rapid onset of symptoms • Symptoms are visible and easily related to food • Usually supportive diagnostic tests • Skin prick tests, specific IgE often positive • Open food challenge easy to interpret • Difficulties mainly occur if complex mixture of food antigens ingested
Contrasting difficulty in non IgE-mediated food allergy N =14 • Often delayed onset symptoms • True association missed • Symptoms often chronic • Eczema, loose stools, ± poor weight gain • Motility disturbance - colic, reflux, constipation • Tests often negative • Skin prick tests, specific IgE • Skin patch tests – variable reports N = 4 Hill et al, J Pediatr 1999
Cow’s milk sensitive enteropathy • T cells become milk-sensitised • Causes villous shortening, crypt lengthening • Variable antibody response • Epithelial function impaired • Lactose malabsorbed • Protein, fat malabsorption less striking • Barrier function ↓ - 2o sensitisations
Reflux or milk allergy? • The screaming back-arching baby almost always is milk allergic – not simple GOR • Even more likely if the baby has: • Eczema, cradle-cap • Colic • Red swollen anus • Nappy rash • Candida • Prolonged viral infections • FH of atopy, autoimmunity (ask about thyroid disease)
Causes of milk allergy • Impaired oral tolerance mechanisms • Loss of previously acquired tolerance • Often pathogens break epithelial barrier • eg Cow’s milk allergy after rotavirus • Secondary sensitisation to soya etc • Failure to establish oral tolerance initially • Immunological abnormalities • Inadequate innate immune exposures • eg breast-milk sensitisation, multiple food allergy
Oral tolerance • Dependent on the gut flora • Innate immune responses to flora are critical • Mediated by regulatory T cells (TREG) • Different mechanisms for low and high doses • High doses – induce anergy of T cells • Antigen presented by the epithelium • Low doses – require active TREG generation • Antigen taken up in lymphoid follicles
Diagnosis of CMSE • Depends on clinical recognition • Skin prick test -ve • Specific IgE -ve • Features include: • Post prandial distension, acid stools • Weight gain often impaired • May have eczema, colic, dermatographia • Micronutrient deficiencies
Sir Samuel Gee The first modern description of coeliac disease 'chronic indigestion met with in persons of all ages, Yet especially apt to affect children between 1 and 5 years old‘ Lecture at GOS, 5th October, 1887
Diagnostic aids • Antibodies • Anti-gliadin – moderate sensitivity- not specific • Anti-reticulin – possibly more specific • Anti-endomyseal/ TTG – sensitive and specific • HLA association • B8 – first described • DR3 or DR5/7 - Much more predictive • DQ2/DQ8 – actual association
Coeliac disease Farrell and Kelly, NEJM 2002
Limitations of biopsy • Changes may be non-specific. • Similar appearances in other diseases • Lesion may be patchy • Capsule biopsies are jejunal, endoscopic are not • Possibly less marked in D2 and D3 • May even be absent in D2/3.
IBD in childhood • Rising incidence and change in phenotype • Advances in genetics • Immunological basis • Inflammation required to establish tolerance • The central role of the gut flora • Pointers from epidemiology • IBD and the “Clean-Child” hypothesis
Dalziel’s report BMJ 1913 • Autopsies on 13 patients with intestinal obstruction • Inflamed jejunum, ileum or colon in all • Transmural inflammation seen on histology
“Crohn’s disease” • Weiner 1914, Moschowitz & Wilensky 1923, 1927, Goldfarb & Suissman 1931 • Ginzburg & Oppenheimer(for Berg) 1927,1928 • Ginzburg & Oppenheimer with Crohn. May 2, 1932, AGA • Crohn. May 13 1932, AMA Crohn BB, Ginzburg L, Oppenheimer GD. Regional ileitis: A pathologic and clinical entity.J Am Med Assoc 1932; 99: 1323 – 1328.
Crohn’s or UC • Crohn’s – Transmural. Focal chronic inflammation. Fibrosis. Granulomas. Anywhere along GI tract. Th1 response. • UC – Largely mucosal. Diffuse acute and chronic inflammation. Essentially confined to colon. • Indeterminate colitis. Definite IBD. Features between UC and Crohn’s. May evolve with time.
IBD incidence • Highest Scandinavia, Scotland • Increased incidence on migration from low to high-risk countries • Indian subcontinent origin in UK • Ethnic groups • Ashkenazi Jews
IBD susceptibility genes • European twin-birth registries • Concordance for CD: MZ 37%, DZ 7% • Concordance for UC: MZ 10%, DZ 3% • Susceptibility loci from genome-scanning • IBD1 – chromosome 16. CD. NOD2 gene • IBD2 – chromosome 12q. UC > CD • IBD3 - chromosome 6p. MHC locus • IBD4 – chromosome 14q. CD
IBD – breakdown of tolerance to the normal gut flora • Enteric bacteria provide continuous immune challenge • Evidence of specific unreactivity to own flora • This is lost in active IBD • Flora reactive T cells, antibody • Reaction to normal flora causes experimental IBD
Paediatric inflammatory bowel disease • Similarities to adult IBD • Essential inflammatory processes • Mucosal lesion • Differences to adult IBD • Management emphasis • Growth, puberty, psychosocial • Indications for steroids, surgery
Patterns of Paediatric IBD • “Classical” Crohn’s disease and UC • CD now becoming more prevalent • Marked increase in incidence • Ileocaecal involvement most common in CD • Oral (/anal) Crohn’s • Indeterminate colitis
Aims of management • Minimise impact of disease on: • Linear growth • Psychosocial development • Pubertal development • The family • ie Multidisciplinary specialised therapy
Diagnosis • Clinical assessment • exclude infectious aetiologies • Upper endoscopy • Colonoscopy (incl. ileoscopy) • +/- Barium follow-through/ MR enteroclysis
Mucosal healing • Minimal • Steroids, Mesalazine, Antibiotics • Slow but definite healing • Enteral nutrition, Azathioprine, 6MP • Rapid but definite healing • Infliximab, adlimumab
Mucosal healing • Only 29% of patients with colonic Crohn’s disease heal with corticosteroids • Role of enteral nutrition • Healing with azathioprine • 70% heal with Infliximab • single infusion improved histology / mucosal inflammation
Current success... • Induction of remission • 75-85% within 2-4 weeks • Maintenance of remission • 60-70% relapse at 12 months • 30% steroid dependent • but..40-70% in remission on Aza at 12 months
IBD Therapies • Aminosalicylates • Nutrition • Antibiotics • Corticosteroids • Immunosuppressants • Immunologic • Surgery
Steroid therapy • Avoid when possible in children • Poor effect on mucosa • Second line agent • relapsing disease • severe exacerbation (i.v. hydrocortisone) • Reducing course 2mg/kg (max 60mg / day)
Highly effective first-line therapy Polymeric formulas more palatable Reduce pro-inflammatory cytokines Increase regulatory cytokines Animal models suggest alteration of gut flora Motivation of child and family critical Enteral nutrition in paediatric IBD
Infliximab safety • Short-term • infusion related • Medium term • infectious complications • delayed hypersensitivity • antibody formation • Long-term • Malignancy – Hepato-splenic T cell lymphoma