Download

1 / 35
360 likes | 527 Views
Lactose intolerance. Antonio Cao. Mauro Congia. Dipartimento di Scienze Biomediche e Biotecnologie Università di Cagliari ASL Nº8 Via Jenner, 09121 Cagliari. Curriculum Vitae Mauro Congia, M.D. 1) Dati Personali Data di nascita:16, Giugno 1957 Luogo di nascita:Cagliari.

E N D
Lactose intolerance Antonio Cao Mauro Congia Dipartimento di Scienze Biomediche e Biotecnologie Università di Cagliari ASL Nº8 Via Jenner, 09121 Cagliari
Curriculum Vitae Mauro Congia, M.D. 1) Dati Personali Data di nascita:16, Giugno 1957 Luogo di nascita:Cagliari 2) Attuale Indirizzo Dipartimento di Scienze Biomediche e Biotecnologie (DSBBT), Università di Cagliari Via Jenner, 09121, Cagliari, Italy Phone: +39-070-609 5522: Fax: +39-70-609-5558 3) Corso di studi -Laurea in medicina e chirurgia nel 1982 con 110 e dichiarazione di lode. -Specializzazione in Pediatria nel 1986 con 60/60 e dichiarazione di Lode. -Scuola di Sanità Militare a Firenze nel Gennaio-Aprile 1985 e Ufficiale Medico di Complemento Aprile 1985-Aprile 1986.
Obbiettivi della presentazione • Inquadramento nosologico delle varie condizioni associate alla ipolattasia • Sintomatologia della intolleranza al lattosio, fattori che ne condizionano la variabilità e suggerimenti volti a ridurne la comparsa • Meccanismo di controllo molecolare del promotore e ipotetico meccanismo di influenza sulla trascrizione dell’mRNA del gene della lattasi che potrebbe essere alla base della ipolattasia • Genetica della lattasi, implicazioni evoluzionistiche e prospettive future
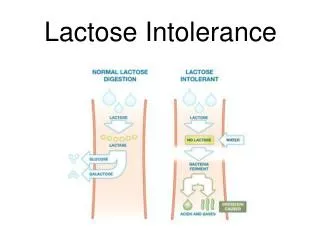
Lactose intolerance Terminological differences and possible confounding terms about lactose intolerance • Hypolactasia(lactase nonpersistence, lactase restriction): means that there is low lactase activity in the jejunal mucosa • Normolactasia(lactase persistence): means that there is persistent lactase activity comparable to the neonatal period • Lactose maldigestionand lactose malabsorptionare terms to describe a poor lactose hydrolysing capacity without symptoms • Lactose intoleranceshould only be used for a clinical entity, describing symptomatic lactose maldigestion (20% of hypolactasic individuals)
Hypolactasia • The gene is located in 2q21 Lactase domain Phlorizin hydrolase domain • 17 Exons (49 Kb) • 6 Kb mRNA • 1927 Amino acids
Hypolactasia It is due to low levels of lactase-phlorizin hydrolase (LPH) in the brush border of the small-intestinal enterocytes. • -glucosidase activity responsible for hydrolyzing phlorizin, a disaccharide found in roots and bark of plants of the family Rosaceae and some seaweeds Lactase has two activities: • -galactosidase activity -1,4- galactosidic linkage Lactase Lactose Galactose Glucose
Hypolactasia Physiological factors involved in lactose absorption • LACTOSE DIGESTION It is the rate-limiting step in the overall process of absorption Enzyme activity is greatest in the mid- jejunum, decreasing both proximally and distally, resulting in minimal activity in the proximal duodenum and the terminal ileum • Lactose is hydrolyzed • Uptake of glucose and galactose is accomplished by the sodium-dependent glucose carrier • Defects in this transporter result in severe diarrhea following carbohydrate intake
Hypolactasia Lactase activity is high during infancy, when milk is the main nutrient and in the vast majority of humans decline with aging The switch is genetically determined despite a continued intake of lactose
Hypolactasia Lactase deficiency may be primary or secondary Three forms with primary deficiency of lactase are recognized: • Congenital lactase deficiency (Rare) • Developmental lactase deficiency (Prematurity) • Adult lactase deficiency(Very common)
Hypolactasia A forth condition of lactose intolerance having serious consequences in infants but associated with a normal presence of lactase in enterocytes is the: • Congenital lactose intolerance Abnormal absorption of lactose and other disaccharides from the gastric mucosa (lactosuria disappears when lactose is given intraduodenally). Vomiting, failure to thrive, dehydration, renal tubular acidosis, aminoaciduria, liver damage, lactosuria and cataracts. A milk-free diet leads to rapid recovery, and after 6 months of age a normal diet (with milk) is well tolerated.
Hypolactasia • Congenital lactase deficiency It is a rare recessive disease Since 1966, 42 patients have been diagnosed in Finland and 18 elsewhere. Usually, the mother notes a watery diarrhea, generally after the first feed of breast milk or at the latest within the next 10 days. Characterized by an almost total lack of LPH activity in jejunal biopsy. No mutation in the lactase gene (LCT) was found in a Finnish patient with congenital lactase deficiency.
Hypolactasia • Developmental lactase deficiency It results from low lactase levels and is a consequence of prematurity Lactase activity in the fetus increases late in gestation: 23rd week 10% of full-term between 25rd and 34rd is 30% of full-term between 34rd and 35rd 70% of full-term Premature infants born at 28 to 32 weeks of gestation have reduced lactase activity
Hypolactasia • Adult lactase deficiency It is the most common form of disaccharidase deficiency The prevalence of primary adult lactase deficiency varies according to race Of the world’s population, 75% is estimated to be lactase-deficient Race: Persons of all races are affected, with higher prevalence among Asian, African, and South American persons. Age of presentation: variable (1-2 years among Thai population to 10–20 years among Finns) Sex: Males and females are affected equally.
Hypolactasia • Symptoms after the ingestion of lactose Lactose intolerance Abdominal pain (crampy, often localized to the periumbilical area or lower quadrant) Bloating Flatulence Borborygmi may be audible to the patient and on physical examination Diarrhea (stools are usually bulky, frothy, and watery) Vomiting (particularly in adolescents) • Variability of symptoms There is a high difference between patients in the perception of symptoms
Hypolactasia • Development of symptoms of lactose intolerance is related to several factors 1. Amount of lactose in the diet 2. Rate of gastric emptying • If gastric emptying is symptoms • Skim milk is more associated with symptoms • Diarrhea following subtotal gastrectomy is often a result of lactose intolerance (gastric emptying is accelerated in patients with a gastrojejunostomy) 3. Small-intestinal transit time. • More rapid small-intestinal transit makes symptoms more likely
Hypolactasia • Lab Studies: Lactose tolerance test Measures serial blood glucose levels after oral lactose load sensitivity of 75% specificity of 96% The diagnosis is confirmed if the serum glucose level fails to increase by 20 g/dL above baseline False-negative results in presence of diabetes and small bowel bacterial overgrowth Abnormal gastrointestinal emptying can also affect the results
Hypolactasia • Lab Studies: Milk tolerance test Administer 500 mL of milk and measure the blood glucose level An increase of less than 9 mg/dL indicates lactose malabsorption Dietary elimination Resolution of symptoms with elimination of lactose-containing food products and resumption of symptoms with the reintroduction are findings suggestive of lactose intolerance. Thus dietary elimination should be used only for diagnosis of lactose intolerance
Hypolactasia • Breath hydrogen test This is the diagnostic test of choice Subjects are administered lactose, after which expired air samples are collected for 3 hours to assess hydrogen gas concentrations A rise in breath hydrogen concentration greater than 20 parts per million over the baseline after lactose ingestion suggests lactase deficiency
Hypolactasia • Small bowel biopsy This is the criterion standard It is invasive and rarely performed Provides definitive information The biopsy results may be normal if deficiency is focal or patchy • Genetic tests They will be available soon. May be based on the detection of C/T polymorphism at position -13910 upstream the LPH gene
Hypolactasia • Secondary lactase deficiency Treatment is directed at the underlying cause • Morbidity It is low and the condition is not lethal • Possible complications Osteopenia in lactase deficiency seems to be a risk factor for osteoporosis (due to avoidance of dairy products or interference of undigested lactose with calcium absorption) Consumption of milk in subjects with lactase persistence has been associated with an increased risk of cataract and of ovarian cancer (galactose may be implicated)
Hypolactasia Strategies that allow lactose maldigesters to successfully incorporate dairy foods into their diets 1. Consume small amounts of lactose-containing foods 2. Chronic/repeated intake of lactose-containing foods allows colonic bacteria to adapt and more efficiently metabolize lactose 3. Co-ingest lactose-containing foods with a meal 4. Consider the form of the lactose-containing food Hard cheeses, chocolate and higher fat milks, and ice cream are well tolerated 5. Eat live culture yogurt 6. Utilize commercially available lactose digestive aids
Hypolactasia • Genetics:AR I II III IV V I II III IV V I II III IV
Hypolactasia • Genetics Sequence and mapping of LPH in 1988 (Mantei et al., Kruse et al.) Fine mapping of LPH in 1993 (Harvey et al.)
Hypolactasia • Genetics and molecular defect transcriptional control LPH gene promoter DNA RNA
Hypolactasia • Genetics: cooperative activation of the LPH promoter • All mammals lactase genes examined so far contain binding sites for transcription factors Cdx2, HNF-1, and GATA in their promoter • A physical association between members of GATA-4 or GATA-5 and HNF-1 results in the cooperative activation of the promoter of LPH • The interaction • occurs through the C-terminal zinc finger and basic regions of GATA-5 and the homeodomain of HNF-1 G H G TATAA promoter G TATAA
Hypolactasia • Genetics • An analysis of Finnish families identified a single base polymorphism 13.9 kb upstream of the human lactase gene that correlates with biochemically assayed lactase non-persistence and restricted the locus to a 47-kb interval on 2q21 • Two variants -13910 and -22018 kb upstream of the lactase gene, initially found in Finnish lactose intolerance families • -13910 was also found in all French, U.S., Italian, Korean and German and African cases • The presence of the same DNA variants in non-persistence alleles in different, distantly related populations together suggests that the persistence variant is old, occurring long before the differentiation of these populations
Hypolactasia • Genetics • the polymorphism could modify a transcription factor binding site (AP2), but the functional significance remains to be defined. AP2 consensus sequence? CCCCAGGC C/C(-13910) T/T(-13910)
Hypolactasia • Genetics: long-range cis-acting regulatory element C/T 13910 G/A 22018 CCCCAGGC AP2? ??
Hypolactasia Distribution of lactase phenotypes
Hypolactasia How to explain the high prevalence of lactase persistence and its geographic distribution? 1) "calcium dependence hypothesis” • lactase persistence is high among Northern European populations. Indeed, rickets and osteomalacia were potent selective factors in the conditions of low solar irradiation characteristic of Northwestern Europe 2) ”milk dependence hypothesis”: • lactase persistence is high among all nomadic populations of sub-Saharan area (Beja in Sudan, Tuaregs in Niger, Fulani in Nigeria, Tussi in Congo basin) • pastoralists in highly arid environments maintain balance of water and electrolytes through plentiful milk supply
Hypolactasia • Genetics geographic distribution All three hypotheses are supported by the geographic distribution of high lactose digestion capacity in adults, but are also confounded by the shared ancestry of the population. In 1997 Holden and Mace, using a comparative method that takes the problem of phylogenetic confounding into account suggested that lactase persistence distribution is consequence of adaptation to dairying. The analysis does not support the hypothesis that lactose digestion capacity is additionally selected for either at high latitudes or in highly arid environments • Thus lactase persistence is an example of Gene-Culture co-evolution Finally using maximum likelihood methods they suggested that the evolution of milking preceded the evolution of high lactose digestion.
Hypolactasia Future prospective: oral gene therapy Few hours after administration, there is widespread and intense gene expression. Enzyme activity persists up to six months after a single application. In a rat model, peroral application of adeno-associated virus encoding -galactosidase (to replace missing lactase) can reverse lactose intolerance. AAVlac after 3 days AAVlac after 6 months Control
Hypolactasia Future prospective: Transgenic animals producing low-lactose milk • Transgenic animals carrying a hybrid gene in which the rat cDNA for LPH was placed downstream a murine mammary -specific promoter • Female mice transgenic for this new gene not only produced lactase in the milk-producing cells, but also secreted it into the milk itself. Milk collected immediately on secretion had 50% less lactose than normal but if it was allowed to collect in the mammary gland, the level dropped even further to around 85% less lactose than usual
Hypolactasia • Conclusions • Hypolactasia is the normal condition while persistence represents the variant • There is no clear evidence for either conditions to predispose to other diseases • People with hypolactasia generally can tolerate about 250 ml of milk without complains • There are many commercially available milks and dairy products containing low amounts of lactose • Lactase enzyme may be added to food containing lactose to increase digestibility of dairy products • A DNA test for for the -13910 polymorphism associated with hypolactasia will be soon available
Riferimenti Bibliografici 1.Jarvela I., Sabri Enattah N., Kokkonen J., Varilo T., Savilahti E. & Peltonen L. (1998) Assignment of the locus for congenital lactase deficiency to 2q21, in the vicinity of but separate from the lactase-phlorizin hydrolase gene. Am J Hum Genet, 63, 1078. 2.Poggi V., Sebastio, G. (1991) Molecular analysis of the lactase gene in the congenital lactase deficiency. Am. J. Hum. Genet, 49 (suppl.), 105. 3.Swallow D.M., Poulter M. & Hollox E.J. (2001) Intolerance to lactose and other dietary sugars. Drug Metab Dispos, 29, 513. 4.Enattah N.S., Sahi T., Savilahti E., Terwilliger J.D., Peltonen L. & Jarvela I. (2002) Identification of a variant associated with adult-type hypolactasia. Nat Genet, 30, 233.