Download
1 / 48
480 likes | 624 Views
The Problem Colleague. Carol A. Burke MD, FACG Cleveland Clinic, Cleveland OH. Objectives. Define professional vs disruptive behavior Discuss scenarios that a “problem colleague” may present to you Develop a strategic plan for approaching a colleague about concerns Discuss impairment issues

E N D
The Problem Colleague Carol A. Burke MD, FACG Cleveland Clinic, Cleveland OH
Objectives • Define professional vs disruptive behavior • Discuss scenarios that a “problem colleague” may present to you • Develop a strategic plan for approaching a colleague about concerns • Discuss impairment issues • Plan an approach for accessing resources needed for a colleague
What Defines Medical Professionalism ? Professionalism is like pornography: easy to recognize but difficult to define Sir Luke Fildes, The Doctor, 1887
Defining Medical Professionalism • Subordinate personal interests to those of others • Adhere to high ethical and moral standards • Respond to societal needs with behaviors reflecting social contract with communities served • Evince core humanistic values, honesty and integrity, caring and compassion, altruism and empathy, respect for others, trustworthiness Swick H. Acad Med 2000; 75
Defining Medical Professionalism • Exercise accountability for self and colleagues • Demonstrate continuing commitment to excellence • Exhibit commitment to scholarship and advancing the field • Deal with high levels of complexity and uncertainty • Reflect upon actions and decisions Swick H. Acad Med 2000; 75
ABIM and Professionalism • Since 1994, ABIM has required candidates to demonstrate they have acquired the values of professionalism • ‘‘aspires to altruism, accountability, excellence, duty, service, honor, integrity and respect for others
AMA Principles of Medical Ethics Physician must recognize responsibility to patients first and foremost, as well as to society, to other health professionals, and to self. Principles adopted are standards of conduct defining essentials of honorable physician behavior II. A physician shall uphold the standards of professionalism, be honest in all professional interactions, and strive to report physicians deficient in character or competence, or engaging in fraud or deception, to appropriate entities IV. A physician shall respect the rights of patients, colleagues, and other health professionals, and shall safeguard patient confidences and privacy within the constraints of the law. AMA Code of Ethics
Disruptive Behaviors • Profane, disrespectful or demeaning language or behaviors • Sexual harassment • Intimidation • Uncooperative attitudes • Failure to follow practice guidelines or practice standards • Verbal or physical outbursts of threats • Criticizing hospital staff in front of patients or other staff • Negative comments about another providers care • Boundary violations: staff or patients • Unethical or dishonest behavior Leap L., Ann Intern Med. 2006;144:107-115.
Joint Commission Regulations on Disruptive Behaviors • 2008, JC required hospitals to have a code of conduct and process for managing disruptive and inappropriate behaviors • “overt actions such as verbal outbursts and physical threats, as well as passive activities such as refusing to perform assigned tasks or quietly exhibiting uncooperative attitudes during routine activities” • “intimidating and disruptive behaviors are often manifested by health care professionals in positions of power. Such behaviors include reluctance or refusal to answer questions, return phone calls or pages, condescending language or voice intonation and impatience with questions.” http://www.jointcommission.org/SentinelEvents. Iss. 40, Behaviors that undermine a culture of safety. 2008
The Disruptive Physician Engages in consistent pattern of unprofessional, uncooperative or contentious behavior which creates a hostile and demoralizing work environment, contributes to poor patient outcomes and compromises the delivery of safe and quality care
Characteristics of Disruptive Physicians • Don’t think of themselves as disruptive • High achievers • Expect high standards, of self and others • See themselves as patient advocates • Well liked by their patients • Passionate about their work • Appear confident • Believe in what is right • Often neglect their own health and wellness • Feel distressed, frustrated, disillusioned • All or nothing thinking Modified from Jeffrey Kolson
Characteristics of Disruptive Physicians • Legitimate concerns communicated ineffectively • Feel under appreciated or unrecognized • Poor team players, preferring to act alone • Communicate emotionally, poor control over anger • Easily offended, fragile ego • Distrust and suspicious of motivation of others • Lack respect or empathy of others • Rarely apologizes for behavior, blames others • Passive aggressive Modified from Jeffrey Kolson
Factors associated with Disruptive Behaviors • Illness, age, disease-related cognitive impairment • Failure to maintain or acquire knowledge and skills • Overwork, lack of sleep, family strife
Factors associated with Disruptive Behaviors • Rapidly changing work environment • Lack of control, Inadequate systems support • Supervisor pressure, productivity demands, cost containment requirements, malpractice litigation • Poor practice management skills • Challenges with poorly performing colleagues or providers chronic criticisms creating difficult practice environments
Institutional Factors • Disruptive behavior sometimes reaction to legitimate problems with system • Lack of clear or enforced code of conduct • Code of silence • Fear of confrontation, retribution, lawsuit, physical safety • Fear of damaging physicians career
Factors associated with Disruptive Behavior • Mental problems, substance abuse or dependence • Associated with MD suicide • Workplace often last affected by DB due to above • Non professional MD relationships already “impaired” • Addiction reported in > 50% MDs admitted to psych hospitals • Higher frequency of ETOHism in female MDs than women in general population Leap L., Ann Intern Med. 2006;144:107-115
Factors associated with Disruptive Behavior • MDs who suicide more critical of others/selves and blame self for illness • Some evidence MDs uncomfortable seeking help, instead resort to alcohol or drugs and isolation • Once help sought, appears not taken seriously by colleagues • Among suicidal physicians who sought help, > 50% who committed suicide diagnosed with psychiatric conditions but not hospitalized before death Leap L., Ann Intern Med. 2006;144:107-115
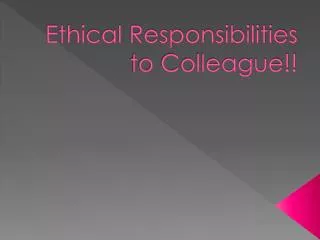
Physician Suicide Rates MenWomen 2.27 1.41 Schernhammer ES, Am J Psychiatry 2004; 161:12
Impact of Disruptive Behavior • Poor adherence to practice guidelines • Loss of patients • Low staff morale and turnover • Decreased staff and patient satisfaction • Medical errors, adverse outcomes, malpractice claims • Association between patient complaints and MDs risk management profiles • Consistently doctor-patient, doctor-doctor, and staff-doctor communication is disruptor of team function and driver of risk management activity
Communication • Hierarchy, or power distance, frequently inhibits people from speaking up • Effective leaders flatten the hierarchy, create familiarity and make it feel safe to speak up and participate. Leonard M, Qual Saf Health Care 2004;13(Suppl 1):i85–i90.
Positive impact of managing disruptive behaviors • Improved staff satisfaction and retention • Enhanced reputation for the practice • Creation of a culture of professionals who are role models for trainees and one another • Improved patient safety • Reduced liability exposure and risk management activity • Greater productivity, civility and desirable work environment
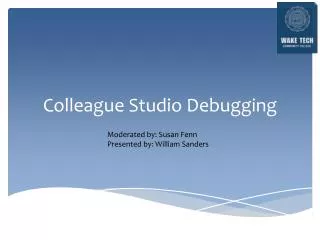
Frequency and Impact of Disruptive Behavior 4530 participants, 2846 nurses, 944 MDs, 40 administrators, 700 other Rosenstein A, Joint Comm J Qual Patient Safety 2008;34
Prevalence of Disruptive Behaviors • Interns versus Staff • Condescending behavior (OR, 5.46; P < .001) • Exclusion from decision making (OR, 6.97; P < .001) • Berating (OR, 4.84; P = .02) • Inappropriate jokes, abusive language, and gender bias (NS) • Interns: RN most frequent source of disruption (OR, 10.40; P < .001) • Staff: Other MD most frequent source of disruptive behaviors Mullan CP, J Grad Med Educ. 2013; 5(1):25-30
Approach to Disruptive Behavior First Steps Next Steps Educate team on behaviors and code of conduct Hold members accountable for modeling desirable behaviors Implement processes appropriate for the organization Provide training for leaders in relationship-building, collaborative practice, skills for giving feedback on unprofessional behavior, and conflict resolution • Develop code of conduct defining acceptable, disruptive and inappropriate behaviors • Devise policies and procedures for identification and management of DB
Approach to Disruptive Behavior Develop, implement a reporting/surveillance system Use tiered, non-confrontational interventional strategies Conduct interventions in context of organizational commitment to health and well-being of all staff, patient safety and quality of care Ensure resources to support individuals whose behavior is caused or influenced by physical or mental health issues Document attempts to address disruptive behaviors
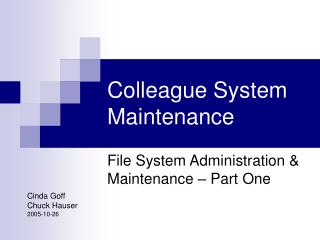
ACTION Dismissal Authority intervention Awareness intervention One on one intervention Increasing Severity of Behavior Unacceptable behavior under any circumstance or repeated misconduct Pattern persists or worsens Repetition of same type of misbehavior: A pattern of such develops Single, non-violent or non serious incident Modified from: Hickson GB. Acad Med 2007;82(11):1040-8
Management of Disruptive Behavior • Timely • Objective and factual • Organized • Role specific • Confidential • Respectful • In best interest of patient, MD and Institution • Measure it
Measuring Disruptive Behavior Pichert J, Advances in Patient Safety: New Directions and Alternative Approaches (Vol. 2: Culture and Redesign). Rockville (MD): Agency for Healthcare Research and Quality (US); 2008 Aug
Collegial Approach • Preferred method, for as long as possible • Non confrontational, non punitive, respectful • Use with behaviors that don’t require reporting • Present objective observations/concerns • Affirm value to institution and acknowledge their aspirations • Provide feedback on impact of behavior
Collegial Approach • Point out need for change • Suggestions process/dealing with frustration • Offer voluntary referral for additional resources • Initiate documentation and continue monitoring • If problem persists, provide warning/consequences
Strategies • Goal: Immediate intervention to diffuse tension and de-escalate disruptive reactions • “ I observed what occurred and …” • “ I’m concerned about what is occurring…” • “ I sense a significant amount of frustration on your part…” • “I saw some behaviors that concern me greatly…” • “It seems like the situation has deteriorated…”
Strategies • Immediate feedback • Limit setting • Empowerment of the target as focus • Respectful communication is attempted with clear expectations for appropriate behavior. Requires assertiveness • “I am going to ask you to refrain from using that language with me…” • “I cannot help you if you continue to yell at me…” • “This behavior is unacceptable and unnecessary…” • “STOP”
Strategies • Explore root causes, underlying emotions, needs • Please tell me more about how things got to this point….. • I hear you say you feel frustrated because…. • I see you have been unable to achieve what is important to you ….. • Avoid validating ineffective behaviors
Strategies • Acknowledge current behavior not effective • “ It seems like despite your efforts, the situation has gotten worse…” • “In retrospect, would you do it again the same way?” • “It sounds like you recognize your approach needs to change….” • “I think it is clear things cannot continue this way…”
Strategies • Provide feedback, clarify procedures, offer possible solutions. When possible let MD decide next step toward change • “I really appreciate your knowledge and expertise, at the same time, I wonder how you might improve on the way you communicate without getting so angry…” • “I need you to consider how our procedure works….” • “ It is evident to me that your goal to become a physician leader requires development in certain areas…” • I would really like you to consider meeting privately with the PHP to strengthen in these areas…”
Peer Messengers • Peer messengers, recognized by leaders, supported with ongoing training, high-quality data, and evidence of positive outcomes, willing to intervene with colleagues over extended time Pitchert J, Jt Comm J Qual Patient Saf.2013 Oct;39(10):435-46
Impact of Peer Messengers • 178 peer messengers and 373 high risk MDs • 97% high-risk MDs received feedback • 64% "Responders” • Risk scores improved > 15% • Nonresponders scores worsened 17% or remained unchanged 19% (p < 0.001). Pitchert J, Jt Comm J Qual Patient Saf.2013 Oct;39(10):435-46
Impact of Peer Messengers • Responders Characteristics: • Practicing medicine and surgery vs emergency medicine • Longer organizational tenures • Lengthier first-time intervention meetings • Years to achieve “responder” correlated with communication-related complaints (r = .32, p < .001), but all complaint categories equally likely to change • CONCLUSIONS: Peer messengers reduce patient complaints, are adaptable to address unnecessary variation in other quality/safety metrics. Pitchert J, Jt Comm J Qual Patient Saf.2013 Oct;39(10):435-46
Formal Approach • Necessary when conduct unresolved or egregious • Verbal or physical assault • Adverse effect on patient safety, well being • Document facts in writing, confidential • Consult with legal, professional staff affairs • Meet MD with coordinated and clear objectives • Set agenda, focus on behavior • Avoid root causes, shifting focus, displaced blame
Formal Approach • Avoid mixed messages • Review code of conduct • Identify behavioral expectations and consequences • Affirm commitment to help the MD • Review disciplinary steps • Inform of referral to Professional Affairs • Fitness for duty • Document meeting, monitor, continue FU’s Modified from Jeffrey Kolson
Strategies • Immediate cessation behavior, non negotiable • Formal description of problem provided and remediation options reviewed, affirm confidentiality • “We are investigating reports you have violated our code of conduct…” • “Continued actions of this nature will not be acceptable….” • “This matter will require your full cooperation to resolve…” • “We would like to offer you the opportunity to rectify this situation…” • “Failure to rectify will result in further disciplinary action…”
Treatment Modalities • Role Modeling, Coaching, 360 evaluation • Psycho-Education, Group Therapy • Psychologic Counseling, Psychiatric Treatment • Substance Abuse/Dependency Treatment • Education and training • Phone etiquette or “charm school” • Sensitivity or diversity training • Stress and anger management • Conflict management or assertiveness training • Communication competence
Summary • Standards for appropriate behavior exist • Disruptive Behavior is common, unacceptable • Organizational commitment, education and resources required • Devise policies for recognition/management of DB • Tiered approach to intervention • Collegial approach first • Explore root causes, provide support, set consequences