Download
1 / 8
140 likes | 748 Views
FEMUR FRACTURES. Common injuries. May be due to direct or indirect trauma. Signify significant trauma. Most common cause; M.V.A. Commonly closed fractures. CLASSIFICATION. Many ways of classifying femur fractures.

E N D
FEMUR FRACTURES. • Common injuries. • May be due to direct or indirect trauma. • Signify significant trauma. • Most common cause; M.V.A. • Commonly closed fractures.
CLASSIFICATION. • Many ways of classifying femur fractures. • The easy way is to classify them ANATOMICALLY. This classification is relevant in terms of treatment : • Proximal femur ; intracapsular ( neck #’s) , intertrochanteric and subtrochanteric. • Femoral shaft fractures. • Distal femoral fractures ( supracondylar and intra-articular).
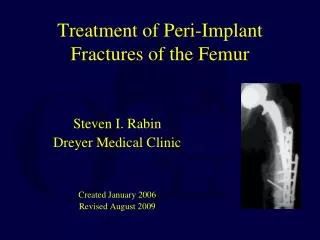
PROXIMAL FEMUR FRACTURES. • FEMORAL NECK FRACTURES. • Intracapsular fractures. • Caused by severe trauma especially in young patients. • The most important complication is avascular necrosis. • They are emergencies. • They should always be managed or treated surgically.
CLASSIFICATION OF N.O.F. #’S. • Classified according to Garden ; Garden 1 : incomplete fractures. Rx= fixation in situ. Garden 2 : complete but undisplaced fracture. Rx = internal fixation. Garden 3 : displaced fracture but there is still contact . Rx = reduction and fixation. Garden 4 : completely displaced fracture .Rx = depends on the age of pt., activity level and the general condition. Options ; reduction and internal fixation, hemi-arthroplasty or total arthroplasty.
INTERTROCHANTERIC #’S. • May follow trivial trauma ; old patients. • Strong abductors tend to cause significant displacement. • The limb is shortened , abducted and externally rotated. • If not fixed surgically , the limb will unite in this fashion. • They are best treated by ORIF.
SUBTROCHANTERIC #’S. • The fracture is within 5 cm of the lesser trochanter. • The abductors and flexors of the hip tend to cause flexion , abduction and external rotation of the proximal fragment. • Difficult to obtain and maintain reduction. • These fractures are best treated by ORIF.
FEMORAL SHAFT #’S. • The shaft lies between the subtrochanteric ( 5 cm below the lesser trochanter) and the supracondylar areas( 8 cm above the joint line). • There are no predominantly strong muscle group. • Femoral shaft fracture can be successfully managed conservatively ; closed reduction and skeletal traction ; Thomas’ splint.
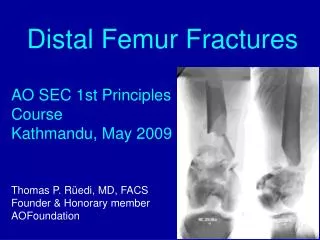
DISTAL FEMORAL #’S. • The gastrocnemius muscle is the deforming force ; the distal fragment is displaced posteriorly. • The fracture tends to angulate posteriorly. • It is difficult to manage conservatively. • The majority are best treated by ORIF. • Those fractures that extend intra-articularly , are managed according to the principles of Intra-articular fractures.