Download
1 / 28
310 likes | 702 Views
Fractures of the Distal Femur Revisited. Joseph Schatzker, MD, BSc presented by Spencer F. Schuenman, DO. Introduction. Intraarticular fxs of the distal femur are serious injuries that result frequently in varying degrees of permanent disability.

E N D
Fractures of the Distal Femur Revisited Joseph Schatzker, MD, BSc presented by Spencer F. Schuenman, DO
Introduction • Intraarticular fxs of the distal femur are serious injuries that result frequently in varying degrees of permanent disability. • The degree of functional loss is often the result of articular cartilage and bone damage, soft tissue injury, or a combination of both.
Historical Perspective • Before the introduction of stable fixation by the AO, supracondylar fxs of the femur most often were treated in skeletal traction because ORIF techniques were very limited. • In the mid 60s, Stewart et al and Neer reported that only slightly more than 50% of patients treated by open means obtained a satisfactory result, whereas closed method yielded satisfactory results in 90% of patients.
The condylar blade plate, was first introduced by the AO in the early 1960s. In 1970 the AO group published its first review of 112 patients with supracondylar fxs. • Of the patients treated surgically, 73.5% achieved good to excellent results-this was revolutionary. • In 1974 Schatzker and colleagues published the Toronto experience with 75% of patients showing a good to excellent result.
Classification • The Comprehensive Classification of Fractures of the Long Bones is an advance on the original AO classification of supracondylar fxs. • Type A: Nonarticular fxs • Type B: Partial Articular • Type C: Complete Articular
Classification cont. • There are further divisions into three subcategories: • Type A1: Simple Type C1:Metaphyseal- • Type A2: Wedge simple • Type A3: Complex Type C2:Metaphyseal- • Type B1: Lateral comminuted • Type B2: Medial Type C3:Comminuted • Type B3: Posterior articular • This information is essential for decision making before surgery and for the correct selection of the implant for internal fixation.
Surgical Exposure • The classic exposure is through a lateral approach that involves the reflection of the vastus lateralis off the intermuscular septum and then a lateral arthrotomy. For C3 fxs, Schatzker and Tile described an approach involving and osteotomy of the tibial tubercle.
Surgical Exposure • For the past 10 or so years, the author has used the total knee approach. • The only time this becomes a problem is if the fracture extends far proximally, but then, the approach described by Henry can be used to expose the entire femur.
Surgical Anatomy • The insertion of fixed angled fixation devices such as the condylar blade plate or the DCS is as far anteriorly as possible along the longest diameter of the elliptically shaped lateral femoral condyle. This line runs approx. 1.5cm-2cm from the distal articular surface.
Surgical Anatomy • The published recommendations for the insertion point along this line have been either the middle of the anterior half of the lateral condyle or the juncture between the anterior and middle 1/3 of the lateral condyle along a line representing its longest diameter.
The further back the insertion point of the angled device, the less well the plate will fit the lateral cortex of the femur. • The reason for this apparent malposition is that the farther back one inserts the fixation device into the distal epiphysis, the wider is the epiphysis in comparison with a corresponding point on the femur. If the plate is secured to the lateral cortex malreduction occurs. This also result in a loss of stability and overloads the medial compartment. If far enough posterior, one can also transect the cruciate ligaments.
Methods of Reduction • An anatomic reduction of the articular component of the fracture continues to be the first step in the reconstruction of any articular fracture. • However, once the epiphysis of a C type fx is reconstructed or if one is dealing with a Type A fx, it is then better to perform indirect reduction as opposed to directly handling the metaphyseal fragments.
The biological price for such a reduction and fixation of the fragments was the devascularization of these fragments. This means a marked delay in the time to union, but more commonly a failure of the fixation unless one did an extensive autogenous bone graft to bridge the zone of fragmentation.
Indirect reduction means that traction is applied either to the limb or directly to the bone by means of a distractor via Schanz screw or plate. • This restores length, rotation, and axial alignment to the metaphysis and diaphysis without any direct manipulation of the bony fragments. • Indirect reduction techniques are therefore biologically superior to direct reduction where the bone fragments are grasped and reduced by open direct manipulation.
Methods of Internal Fixation • The condylar blade plate revolutionized the treatment of supracondylar fractures. • The problem with its use is the multiple guides and reference points and the difficulty in changing its direction or rotation once seated.
To overcome these difficulties, the AO developed the DCS (dynamic condylar screw). Insertion of the screw, however, is much easier because its position in the bone is predrilled with a special triple reamer and its seat is precut with a tap. Furthermore, the reamer is cannulated and is passed over a guide wire and thus, can be checked in the AP plane with a C arm before reaming and can be changed easily. • In addition, if the plate does not fit the shaft of the femur, simple clockwise or counterclockwise rotation of the screw easily corrects the malalignment.
The AO developed the condylar buttress plate for the treatment of C3 fxs. The plate is fixed to the distal femur with 6.5mm cancellous screws. The screw heads are not fixed to the plate and therefore if the bone collapses the screws will move in the screw holes. • If a second plate is used to buttress a multifragmentary fx medially, it must be combined with bone grafting because of the devascularization of the fragments.
The author thinks that an ideal device for the fixation of a comminuted fx of the distal femur is the supracondylar IM nail. This device spans the comminution and acts as an internal bridge with minimal disruption to the metaphyseal fragments. • There are questions about its long-term effects in damaging the articular cartilage especially in young patients. The nail must be seated far enough without any protrusion into the joint space.
Bridge Plating of Multifragmentary Fractures • It has been shown that in comminuted fxs, sufficiently stable fixation is achieved if the fx zone is simply bridged by a plate of adequate strength and length. This is referred to as splinting. The stability achieved by splinting is sufficient to overcome pain originating from the fx. • The plate acts as a splint and as long as viability of the fragments remains, union occurs with the formation of callus.
In fractures with extensive fragmentation and shortening, reduction is best achieved with the use of the large distractor. • It is best to overdistract the fracture. This allows one to tease the fragments with a sharp narrow hook into alignment and reduction.
Open Supracondylar Fracture • The functional outcome of open fxs is largely determined by the degree of their accompanying soft tissue injury. • In stable fixation, infection can be brought under control and a good outcome can be achieved in approximately 80% of the patients. • Major avascular joint fragments covered with articular cartilage are essential to stability and function of the joint, and need to be preserved.
In articular fxs one cannot delay the reduction and fixation, as is often done with the metaphyseal component of the fracture, because articular fragments unite rapidly. • Therefore, one must strive to achieve a atraumatic anatomic reduction of the articular surfaces as soon as possible. • Once the joint is reconstructed the surgeon must decide whether to proceed with the reconstruction of the metaphysis or delay the reconstruction until a stable soft tissue envelope has been achieved.
If there is any doubt as to the ability of the soft tissues to survive a primary reconstruction of the metaphysis, the reconstruction must be delayed. • The metaphysis should then be bridged by either a plate or an external fixator. • It is best not to delay more than 2-3 weeks before converting to another form of fixation. • If there is bone loss, bone grafting should be delayed until approximately 6 weeks from injury. Large bone defects can be filled with antibiotic impregnated cement.
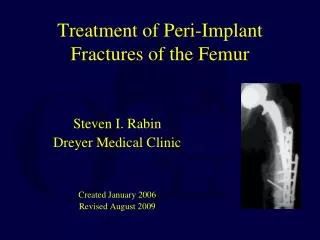
Supracondylar Fracture in the Presence of Total Joint Prosthesis • The author thinks that a supracondylar fracture in the presence of a total knee is an absolute indication for an open reduction and internal fixation. • Treating these fractures by closed means, normal axial and rotational alignment is extremely difficult if not impossible to achieve, yet normal alignment is essential to the long term survival of a total knee replacement.
Before dealing with the fracture, one must establish whether the prosthesis functioned normally and whether the components are solidly fixed. If the prosthesis is stable then fixation can be obtained with a condylar buttress plate laterally and a T-plate medially. • If the fx is complex it is best to secure its fixation with the supracondylar nail. One must be sure that the femoral component can accommodate the nail in the intercondylar notch. If this is not possible, the femoral component must be replaced with a long stem component.
Supracondylar Fractures in Severe Osteoporotic Bone • The most common causes of failure in the elderly patient population are not technical errors but the presence of osteoporosis. • There are certain techniques that one can use to enhance the fixation. If there is a short segment of comminution not greater than 2 - 3 cm in length, it is best to push the small fragments out of the way, shorten and bring the main fragments in contact. This enhances stability, facilitates union, and allows the small fragments to be used as bone graft.
Intramedullary fixation should be used especially if the fx extends over a longer segment. The locking of the nail to the epiphysis can be enhanced with the use of the special flared nuts and also with the addition of bone cement. • If bone cement is implemented, one must make sure that the cement does not enter the fx lines because it will interfere with union of the fragments.
Summary • Despite many challenges and refinements in the surgical treatment of supracondylar fxs since the introduction of the condylar blade plate, these fxs, particularly open and if associated with severe fragmentation of the articular cartilage, or in the presence of osteoporotic bone, continue to be a major unsolved surgical challenge. • The most pressing problems that urgently need solutions are articular cartilage damage and the development of satisfactory methods of fixation of osteoporotic bone.