Download
1 / 49
490 likes | 667 Views
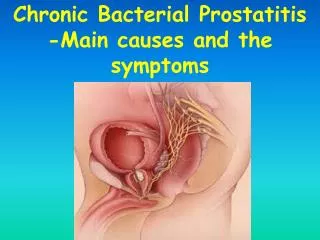
Prostatitis Christian Beck, MD Dortmund Germany. History. First described in 1815 by Legneau. Main treatment was repeated prostate massage. In 1930’s antibiotics came into regular use. Evident that most forms of prostatitis did not respond to Ab’s. Epidemiology (USA).

E N D
History • First described in 1815 by Legneau. • Main treatment was repeated prostate massage. • In 1930’s antibiotics came into regular use. • Evident that most forms of prostatitis did not respond to Ab’s.
Epidemiology (USA) • McNaughton-Collins in 2000 noted 2 million physician visits for ‘prostatitis’ annually from 1990-1994 in USA • Commonest urological diagnosis in men < 50 and 3rd commonest in men > 50, 8% of urology consultations. • Urepik Study 1998 – 35% of men had at least 1 symptom of prostatitis, with 8% describing symptoms as problematic.
Prostatitis: A Major Clinical Problem (Germany) Incidence/prevalence: 4% -11% 8-12% of urologist office visits Life time prevalence 14.8% most common urological diagnosis in men <50 Quality of Life is dismal (depressing) !
Aetiology • Gram –ve enterobacteria account for 90% of acute bacterial prostatitis. (E. coli, Klebsiella, Serratia, Pseudomonas) • Enterococcus (gram +ve) 5 – 10%, and Staphs. • Role of anaerobes are unknown. • Anti-Chlamydial antibodies in 30% of chronic prostatitis, but < 1% culture organism.
Aetiology • Altered Prostatic Host Defence - phimosis; unprotected penetrative anal rectal intercourse; acute epididymitis; indwelling urethral catheters and condom catheter drainage. • Dysfunctional Voiding. • Intraprostatic Ductal Reflux – stones, carbon particles (Kirby et al 1982). • Pelvic Floor Musculature Abnormalities. • Interstitial Cystitis. • Psychological Cause
Investigation • Physical – Signs of infection, abdo tenderness, DRE (anal tone, prostate, pain). • Examination of Urine. • Urodynamics (Video) • Rule out other cause – obstruction, OAB, dyssynergia. • Cystoscopy? • TRUS • Abscess, medial cysts, SV obstruction. • Not diagnostic for Chronic Prostatitis. • Biopsy of no clinical benefit to management.
Examination of Urine • 1968 Meares and Stamey - 4 glass test. • For Chronic Prostatitis only. • Simplified 2 glass test similar sensitivity and specificity to 4 glass test. • 10 WBC’s per HPF is cut off for inflammatory and non-inflammatory category III prostatitis.
Examination of UrineCLASSIC STAMEY 4 GLASS TEST Wagenlehner, F M E; Naber, K G; Bschleipfer, T; Brähler, E; Weidner, W Prostatitis and Male Pelvic Pain Syndrome: Diagnosis and Treatment Dtsch Arztebl Int 2009; 106(11): 175-83; DOI: 10.3238/arztebl.2009.0175
PROSTATITIS DIAGNOSIS Donna R. Coffman, MD Comparison of four-glass and two-glass premassage and postmassage test Nickel JC, Shoskes D, Wang Y, et al: How does the pre-massage and post-massage 2-glass test compare to the Meares-Stamey 4-glass test in men with chronicprostatitis/chronic pelvic pain syndrome? J Urol 176(1):119-124, 2006. The Premassage postmassage test (PPMT) may offer an adequate screening test as an alternative that is simpler, faster, and less expensive than the four-glass test.
PRE-M POST-M Prostatemassage
Category I – Acute Bacterial • Not common • Perineal, external genitalia and suprapubic pain. • Dysuria, frequency and urgency. • Obstructive symptoms. • Febrile illness occasionally with severe sepsis.
Category I – Acute Bacterial The patient typically complains of : • Urinary frequency, urgency, and dysuria. • Obstructive voiding complaints including hesitancy, poor interrupted stream, strangury, and even acute urinary retention are common. Tenesmus. • Perineal and suprapubic pain • Associated pain or discomfort of the external genitalia. • Significant systemic symptoms including fever, chills, malaise, nausea and vomiting, and even frank septicemia with hypotension Approximately 5% of patients with acute bacterialprostatitismay progress to chronic bacterialprostatitis (Cho et al., 2005
Category I – Acute Bacterial • Send MSSU (Mid Stream Specimen of Urine) / blood cultures. • Antibiotics • i.v. if evidence of sepsis • Aminoglycoside, cephalosporins, or fluoroquinolones. • 2 – 4 weeks treatment. • Surgery • SP catheter • TRUSS or CT to exclude abscess. • Abscess best drained by TUR.
Category II – Chronic Bacterial Prostatitis. • 5 – 15% of Prostatitis • Recurrent UTI’s in 25 – 40% • May be asymptomatic between episodes or have a long history of CPPS. • Treat with Antibiotics • Fluoroquinolones (Cipro- Levo- and Ofloxacine) most effective. • 12 weeks of treatment. • 60 – 85% bacteriological cure. • 40% symptom cure.
Category IIIa – Chronic Pelvic Pain Syndrom (CPPS Inflammatory) • Pain – Perineum, suprapubic and penile but can be testes, groin and lower back. • Pain during or after ejaculation. • LUTS (storage and voiding symptoms) • Erectile dysfunction is increased. • Symptoms present for > 3 months. • Sickness Impact Profile – QL scores similar to MI, angina and Crohn’s.
Category IIIb – Chronic Pelvic Pain Syndrom (CPPS non-bacterial) • Same presenting features as IIIa, but < 10 WBCell’s per HPField on Expressed Prostatic Sekretion and VB3. • NIH – Chronic Prostatitis Symptom Index.
Category IV – Asymptomatic Inflammatory Prostatitis • As name suggests!! • WBC’s or bacteria in EPS or VB3 or histological examination of gland. • Present with obstruction, raised PSA, infertility.
Classification: NIH Cat I: Acute Bacterial Prostatitis Cat II: Chronic Bacterial Prostatitis Cat III: Chronic Pelvic Pain Syndrome (CPPS) Cat IIIA: Inflammatory CPPS Cat IIIB: Non-inflammatory CPPS Cat IV: Asymptomatic Inflammatory Prostatitis (AIP) 90%
CPPS Treatment • Antibiotics • Campbells: The Randomized Controlled Trial- try in IIIa and continue if beneficial, no consensus with IIIb. • Nickel et al Urology. 2003 Oct; 62(4) :614-7. RCT comparing Levofloxacin versus Placebo – decrease in NIH-CPSI score, but same as placebo. • De Rose et al Urology. 2004 Jan;63(1):13-6. RCT comparing mepartricin v placebo for 2 months (26 patients). NIH-CPSI scores 60% and 20% reduced. With significant improvements in pain and QoL.
CPPS Treatment • -Blockers • CPPS causes obstructive LUTS. • Campbells – few small studies show improvement in flow and symptoms, esp when combined with Ab’s. No RCT. • Alexander et al Ann Intern Med. 2004 Oct 19;141(8):581-9. RCT of Cipro v Tam v both v placebo = No difference but all caused slight decrease in symptom score. Only 6 weeks • Mehik et al Urology. 2003 Sep;62(3):425-9. RCT of Xatral (Alfuzosin) v placebo for 6 months. Modest but significant reduction in pain and symptom score.
CPPS Treatment • Anti-Inflammatory Agents • NSAID’s improve pain and symptoms. • Nickel et al J Urol. 2005 Apr;173(4):1252-5. RCT of pentosan polysulfate sodium (used for Interstitial cystitis/painful bladder syndrome)versus placebo in CPPS. 300mg TDS for 16 weeks. Slight improvement over placebo, only significant in QoL score.
CPPS Treatment • Hormone Therapy • Nickel et al BJU Int. 2004 May;93(7):991-5. RCT of Finasteride v Placebo slight improvement but not properly powered. • Phytotherapy • Saw Palmetto – no effect • Bee Pollen Extract (a bioflavonoid) showed slight improvements.
CPPS Treatment • Prostate Massage • Campbell’s no good evidence to support use. • Perineal or Pelvic Floor Massage or Myofascial Trigger point release • What? • Cornel et al Eur Urol. 2005 May;47(5):607-11. Epub 2005 Jan 22. RCT of biofeedback showed significant reduction in NIH-CPSI scores. • Other smaller studies give similar results.
CPPS Treatment • Balloon dilatation and needle ablation – some benefit in small series, none properly controlled. • Microwave therapy • 3 studies comparing MT v sham. All showed benefit over sham. 1 study showed 75% improvement with MT, but sham gave 52% improvement. • TURF therapy (TEMPRO) • My study presented on WCE in Munich (Oktober 2009) showed 43% improvement.
CPPS Treatment • Surgery • TURP/BNI only if evidence of obstruction. • TURP in refractory Cat. II reported. • TURP in CPPS – no evidence • Radical prostatectomy – one case reported ‘No definitive clinical series or long-term follow-up has ever been presented, and this type of surgery should not be encouraged or recommended at this time’.
Intraprostatic injection in prostatitis cathegory IIIa And IIIb(CPPS) • Antibiotics • Zinc • Periprostatic BOTOX • Antibiotics and esracain • Antibiotics and steroids ROUTS OF INJECTION Transrectal Perineal transurethral Us guided
Intraprostatic injections Possible side effects • Pain • Hematuria • Dysuria • Hemospermia
HYPERTHERMIA How to convey heat to the prostate: Transrectal (microwave) Transurethral (microwave) Interstitial (laser, Nanoparticles) Tempro or Tuna (radiofrequency) Hifu (ultrasound) All treatments cause some degree of prostate tissue denaturation and if high temperatures are achieved, even tissue necrosis
TURF • Thermotherapy 48 - 53,5° c • No cooling needed
TURF MECHANISM – Principle of Operation RF produces electromagnetic radiation with oscillating electrical and magnetic fields. The design of the antenna seems to affect the heating pattern more than the wave frequency does. Heat is produced while the radiowaves are absorbed by the tissue.
LOCAL EFFECT OF TURF • heating in excess of 50°C is followed by coagulation necrosis • Histopathological effect of thermotherapy appears to be related to the induction of cell death • induced necrosis was shown to disrupt periurethral -adrenergic receptors reflecting denervation of smooth muscle cells consisting with the increased urinary flow rate after TURF • It was demonstrated that TURF increased the sensory threshold (Schwelle) in the posterior urethra by 30%, resulting in the reduction of irritative symptoms
60 Heating point center Heat Distribution For BPH: 55 to 60°C For Prostatitis: 48 to 53,5°C (depending on Age)
Heating Point Balloon Heating Point Center
Contraindications for TURF • Urinary Tract Infektion • Penile implants • Artificial sphincter • Urethral stricture • Previous prostate surgery • Leriche syndrome (is atherosclerotic occlusive disease involving the abdominal aorta and/or both of the iliac arteries). • Prostates under 30 gr or over 100gr.
Treatment Protocol for Prostatitis Insertion of catheter (containing the Applicator) Inflation of catheter balloon & repositioning of catheter Temperature is raised to 39° C (for at least 3 min) than gradually raised to 48 or 53,5°C for additional 57 min. Following treatment - immediate removal of catheter (post-treatment catheter insertion is optional) Interval between treatments: min. 1 month
Is prostatitis a premalignant lesion Prostate carcinogenesis and inflammation: emerging insights Patrick j. et al., Carcinogenesis 2005 26(7):1170-1181
Is prostatitis a premalignant lesion Review Nature Reviews Cancer 256-2692007 Inflammation in prostate carcinogenesis Angelo M. De Marzo, Elizabeth A. PlatzSiobhan Sutcliffe, Jianfeng Xu, Henrik Grönberg, Charles G. Drake, Yasutomo Nakai, William B. Isaacs & William G. Nelson