Download
1 / 1
20 likes | 285 Views
Emery-Dreifuss Muscular Dystrophy- Case report and discussion of pregnancy complications N Aedla, A Duncan Princess Royal Maternity Hospital, Glasgow , UK. OPTIONAL LOGO HERE. OPTIONAL LOGO HERE. Introduction. Antenatal. Conclusions. Delivery.

E N D
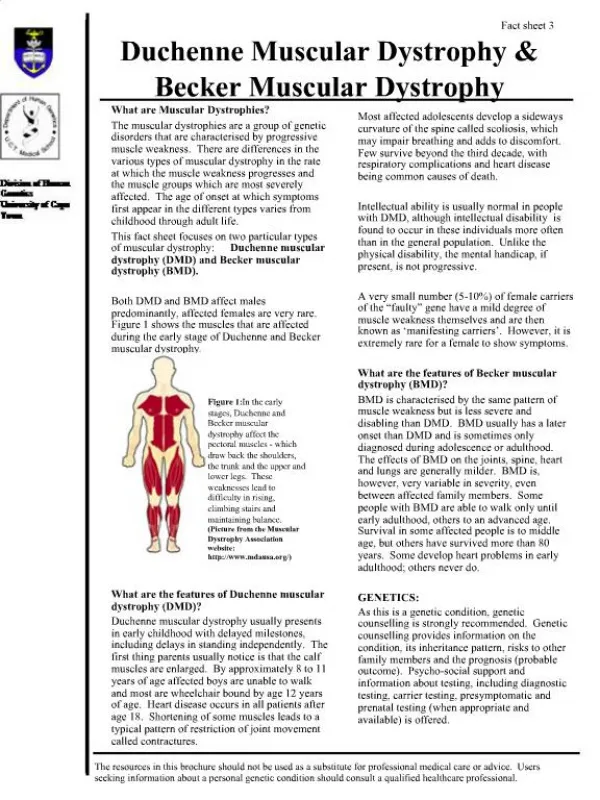
Emery-Dreifuss Muscular Dystrophy- Case report and discussion of pregnancy complications N Aedla, A DuncanPrincess Royal Maternity Hospital, Glasgow , UK OPTIONALLOGO HERE OPTIONALLOGO HERE Introduction Antenatal Conclusions Delivery She was delivered by an elective Caesarean section under combined spinal epidural with dosage of drugs adjusted to her BMI. A male baby weighing 1.04 kgs was delivered with Apgars of 9 at 1 and 9 at 5 minutes. He showed signs of chronic respiratory distress and required ventilation. Placental histology confirmed changes specific to pre-ecclampsia. Her thromboprophylaxis was changed to Warfarin tabs. She had a wound haematoma complicated by a wound infection which was treated with Clindamycin (Penicillin sensitivity). She was discharged home after 1 week. Her antihypertensive medication was stopped at 3 weeks. The baby tested positive for muscular dystrophy gene variant. He remains well to date with support of oxygen at home and has shown development appropriate to age. EDMD requires specialist input via multidisciplinary team. These people are at a high risk of death due to cardiac events and therefore need to optimise their condition prior to conceiving. Aggravation of symptoms is common in early onset and progressive myopathy.2 These women have a good quality of life given the advances in recent medicine. It is therefore not surprising that we will encounter more complicated medical conditions with pregnancies in the future. They must be offered genetic counseling and pre-implantation diagnosis so they are aware of the inheritance and risk to the pregnancy. Due to the rarity of such conditions case reports are useful in parting knowledge and experience to manage such cases. Emery-Dreifuss muscular dystrophy (EDMD) is characterised by changes in certain skeletal muscles and early contractures of the neck, elbow, Achilles tendon and cardiac conduction defects.1 In 1999 Bonne et al., reported diseases caused by mutation in LMNA encoding A-type lamins include autosomal dominant MD and related disorders.1 The incidence is rare and literature sparse on management and optimal delivery plan of pregnant women with this condition. We present one such case and challenges in her management during pregnancy and delivery A 26-year old booked in her first pregnancy at 11 weeks of gestation. She measured 145cm in height and 35 kgs in weight with a BMI of 16. She mobilised using a specialised wheel chair and lived with her partner with a stair lift at home. She was diagnosed as a child with autosomal dominant EDMD. She sought help from assisted conception services and received Letrozole for ovulation induction. She embarked on this pregnancy as she had a good quality of life and was well aware of the risk of inheritance of this condition. She declined pre-implantation genetic counseling. Her myopathy and contractures mainly involved the limb girdle. She also had severe scoliosis of the spine. She attended cardiology regularly due to the high risk of a cardiac event in association with LMNA type-A&C mutation which tested positive in her case. A dual chamber automated implantable cardiac defibrillator was inserted a year ago. She attended the breathing support clinic due to restrictive ventilatory defect with vital capacity of 1.49 litres and 50% of predicted FEV1 with FEV1/FVC ratio of 91%. She stopped anti-depressants (Citalopram and Diazepam tabs) prior to. At booking, she was counseled about the risks with pregnancy and 50% chance of the baby having this condition and high risk of preterm delivery if strain on respiratory or cardiovascular systems. She was commenced on prophylactic thromboprophylaxis (SC Enoxaparin 20mg) daily due to reduced mobility. She was commenced on antihypertensive (PO Labetolol 200mg, BD tabs) as her BP was high at booking (167/104). Subsequently, she had a brief hospital admission for abdominal pain which was thought to be related to her IBS. Her fetal anomaly scan was reassuring at 20 weeks. She required additional antihypertensive and was commenced on 125mg Methyldopa BD tabs. She was seen weekly at the antenatal clinic and required a few admissions with high BP readings. By 26 weeks, she required further addition to her antihypertensive medication and received PO Nifedipine 10mg BD tabs. She was admitted with 2+proteinuria. Her blood results were normal. She received corticosteroid injections (12mg Betamethasone IM, 24 hrs apart) anticipating early delivery. During her inpatient stay she was reviewed by the anaesthetists, paediatricians, physiotherapists and received input from cardiology and cardiothoracic surgeon, respiratory physicians and neurologists. Her defibrillator was switched off. At 28 weeks, her blood urate levels rose at 0.41 and was significantly breathless due to diminished respiratory reserve owing to the gravid uterus. She was discussed at the high risk meeting and we decided to deliver her due to evolving pre-ecclamspia andworsening respiratory reserve. Postnatal Case X-ray Spine lateral view References 1.Bonne G, Di Barletta MR, Vamous S, Becanen HM, Merlini L, Mutoni F, Greenberg CR, Gary F, Urtizberea JA, Duboc D, Fardeau M, Toniolo D, Schwartz K. Mutations in the gene encoding lamin A/C cause autosomal dominant Emery-Dreifuss muscular dystrophy. Nat Genet. 1999;21:285-8 2. Sabine Rudnik-Schoneborn, Beate Glauner, Dorothee Rohrig, Klaus Zerres. Obstetric Aspects in women with fasioscapulohumeral muscular dystrophy, limb girdle musculodystrophy and congenital myopathies. Ach Neurol.1997;54(7):888-894 Chest X-ray (AP view) showing severe scoliosis. Implantable automated cardiac defibrillator seen on left. . Reduced thyromental distance.