Download
1 / 20
210 likes | 474 Views
High School STD Screening: Parental Consent and Confidentiality. Meighan E. Rogers, MPH 2008 National STD Prevention Conference Chicago, IL March 11, 2008. Overview. New York City (NYC) high school STD screening program Scope Results Types of parental consent: Active vs. Passive

E N D
High School STD Screening: Parental Consent and Confidentiality Meighan E. Rogers, MPH 2008 National STD Prevention Conference Chicago, IL March 11, 2008
Overview • New York City (NYC) high school STD screening program • Scope • Results • Types of parental consent: Active vs. Passive • Parental consent processes utilized across US • Confidential screening and result distribution • Addressing parental concerns The findings and conclusions in this presentation are those of the author(s) and do not necessarily represent the views of the CDC/ATSDR.
NYC School Screening Program • NYC: 300,000 high school aged students • Program scope: Target public schools, neighborhoods with high STD rates, ~45% of program schools have school-based health centers (SBHCs) • School wide education, voluntary confidential urine CT/GC testing • Began Spring 2006 - 5 pilot schools • 2007 (Current) school year: • Goal: Educate 30,000 youth, test 15,000 • 7 full time program staff
NYC School Screening Program Results • 2006 school year: • Educated 9500 students (44 schools) • Tested 4,375 (47%) • 209 positive (4.8%); 99% treated • 2007 (current) school year YTD: • Educated 10,561 (~50 schools) • Tested 5178 (49%) • 400 positive (7.7%); 92% treated to date, ongoing
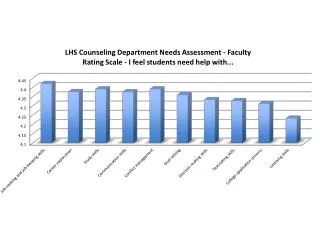
NYC CT/GC Positivity, 2007-2008 * Difference between males & females significant at p<.0001
Approaches to Parental Involvement • Active consent • Passive consent • Notification – parents are notified that the program will take place, are not given option to opt-out
Active Consent – “Opt-in” • Requires all parents to return consent indicating whether they want their child to participate • If consent form not returned, assume refusal Disadvantages: • Lowers response rates/limits participation (40-70%), can limit accuracy, completeness of data and reach • Non-response may indicate disinterest rather than opposition • Costly, time consuming to ensure response
Active Consent (Cont) Disadvantages: • Selection bias- certain groups more or less likely to respond • Under-represents minorities; students of parents with alcohol or substance abuse problems • Over-represents students with higher SES, 2 parent families
Passive Consent - “Opt-out” • Requires parents to respond only if they do not want their child to participate • Non-response is an affirmative response • Secures higher response rates (avg 80-96%) • Ethical method of holding up informed consent principles while securing higher participation Disadvantages: • Non-response may indicate agreement or apathy • Low health literacy, language barriers obstacles to assuring parental understanding
State Laws – STI Services • All 50 states, and Wash DC, allow minors (under age 18*) to consent to STI diagnosis and treatment services without parental consent/involvement • Louisiana and Maryland physicians are allowed to inform the minor’s parents about STI services if in minor’s best interests • SBHCs require parental consent for students to access services, however some will still screen for sexual/repro health services under state law * While no minimum age is specified, a child younger than 12 years would not beconsidered to have the capacity for informed consent
Consent Processes Utilized for School STD Screening Across US • Baltimore: Program conducted through SBHCs • SBHCs agreed to screen/treat for STIs without parental consent, under Maryland state law • New Orleans: Active consent process • School officials and IRB require active parental consent, despite state law • STD program distributes written consent through students • If not returned, parents called by STD staff to elicit consent • Parental consent rates between 50-75%
Consent Processes Utilized for School STD Screening Across US • Philadelphia: City-wide parental notification • Approved as non-research, not reviewed by IRB • Letters, signed by Health Commissioner and CEO of Schools, sent out to parents by schools • NYC: Passive consent process • Despite NYS law, Dept of Ed IRB mandated passive consent • Schools conduct consenting process. If opted out, school responsible for prohibiting student’s participation • Secures high participation rates (Range ~95-100%)
Consent Processes Utilized for School STD Screening across US • Indian Health Service: Consent process dictated by tribe • Minors > 12 able to consent by law, however tribe dictates type of consent required • Most recent tribe required active consent • Consent forms sent home by school • Low participation rates, returned forms mostly declines
Screening – Ensuring Confidentiality • Baltimore/New Orleans: • Testing conducted individually in SBHCs, confidentiality less of an issue, not mass screening • Philadelphia/NYC: • All students participate in education piece, complete demographic info • All students taken to bathrooms for voluntary, confidential testing, all submit test kits (in bag) whether specimen or not • IHS: • Site specific: some sites conduct testing individually Interested in using mass screening Philadelphia/NYC model
Confidentiality of Test Results • Test results only given to individual student • Philadelphia / NYC: Students create a secret password; test results given by phone • New Orleans: • Until 2000, results given personally in sealed envelopes using code numbers • Since 2000, students access results through automated phone system using a PIN and additional access code • Baltimore: Results given to each student individually in SBHC, by Nurse/NP • IHS: Results (positive or negative) given to each student individually by nurse
Parental Involvement • Attend parent association meetings pre-screening to present program, answer questions • Parental Feedback: • Often support STD education, testing • Concerned about confidentiality of testing and treatment • Interested in obtaining test results • Concerned about treatment without their knowledge
Managing Parental Concerns • Describe law preventing dept health staff from sharing test results • Explain that while dept health staff cannot share results, adolescents can share their own results • Encourage parents to have conversations with their children prior to/after program • All students assessed for allergy prior to treatment by NP or MD
Thank you • NYC DOHMH STD Control: Sophie Nurani, Susan Blank, Steve Rubin, Julia Schillinger, Kristen Harvey • STD Screening Program Staff – Public Health Advisors • NYC DOHMH Bureau of School Health • NYC Dept of Education • Fund for Public Health in NY/NY Community Trust Contact Info: mrogers@health.nyc.gov, 212-788-4428