Download
1 / 72
761 likes | 1.14k Views
Nonunions of Long Bones. Robert Probe, MD Scott & White Memorial Hospital Texas A&M University Health Science Center Original Author: Matthew J. Weresh, MD; March 2004; New Author: Robert Probe, MD; Revised January 2007. Definition Epidemiology Etiology Evaluation Classification.

E N D
Nonunions of Long Bones Robert Probe, MD Scott & White Memorial Hospital Texas A&M University Health Science Center Original Author: Matthew J. Weresh, MD; March 2004; New Author: Robert Probe, MD; Revised January 2007
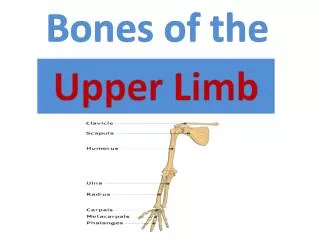
Definition Epidemiology Etiology Evaluation Classification Treatment Principles Stabilization Biologic Specific Bones Clavicle Humerus Forearm Femur Tibia Outline
Definition • FDA: 9 months elapsed time with no healing progress for 3 months. • Problems • Subjective • Arbitrary • Pragmatic: A fracture that has no potential to heal without further intervention
Incidence • Between 5% and 10% of long bone fractures • Relative Risk depends upon: • Injury • Bone • Patient • Treatment
Nonunion under conditions of Absolute Stability • Fracture gaps that exceed the allowable distances for primary or gap healing • Construct instability that prevents primary healing
Nonunion under Conditionsof Relative Stability • Sufficient stability is not imparted at the soft callus stage to allow for mineralization of the chondroid matrix. • Instability prevents bringing bone formation despite biologic activity
Local Risk Factors • Open Fractures • High energy fractures with bone devitalization • Severe associated soft tissue injury • Bone loss • Infection
Systemic Risk Factors • Malnutrition • Smoking • NSAIDs • Systemic Medical Conditions
Smoking and Tibial Fractures Adams Injury 2001
Non-steroidals and Healing • 32 femoral nonunions compared with 67 that healed uneventfully • No difference: • Smoking • Reaming • Locking • NSAIDs • Significant to P< 0.000001 Giannoudis JBJS-B 2000
Iatrogenic • Poor Reduction • Unstable fixation • Bone Devitalization
2 3 4 5 Iatrogenic Stripping • Indiscriminate devitalization (1) • Leads to limited healing potential and implant failure (2,3) • Occasionally requiring resection and reconstruction prior to healing (4,5) 1
Diagnosis Suspected When: • Persistent Pain • Non physiologic motion • Progressive deformity • No radiographic evidence of healing • Failing implants
Clinical Exam • Limb Stability • Limb alignment and length • Condition of the soft-tissue envelope • Neurovascular exam
Radiologic Evaluation • Standard radiographs are often diagnostic • 45 degree oblique films can increase diagnostic accuracy • Despite additional projections, the potential for false-positive results for fracture healing remains
Clinical diagnosis can be confirmed and information about stability obtained with stress radiographs. Varus Valgus
Computed Tomography • Clarity when implants or fracture obliquity produce doubt
Classification • Is there infection? • Is there deformity? • Define the biologic activity and stability
Infection • MRI can play a role in identifying soft tissue component; however, bone edema is too sensitive to be accurate • Reliance on clinical diagnosis augmented by CRP • Low virulence infection may require aspirate or operative culture for diagnosis • Indium scan carries only moderate sensitivity and specificity
Determine Deviations in: • Angulation • Length • Rotation • translation
Define the Level of Osteogenesis along the Spectrum of Biologic Activity hypertrophic oligotrophic atrophic Inherent Biology Weber & Cech: Pseudarthosis, 1976
Nonoperative Treatment • Electromagnetic • Direct Current • Inductive coupling (PEMF, CMF) • Capacitive coupling • Ultrasound • mechanical energy in the form of low frequency acoustic waves 30 mW/cm2
Role of Nonoperative Modalities • All have clinical evidence to support effectiveness • Few comparative studies between modalities • Few comparative studies between nonoperative and operative methods • Best suited for hypertrophic nonunions with good inherent stability • Does nothing to correct deformity or provide immediate stability
Surgical Treatment:Algorithm • Cure infection if present • Correct Deformity if significant • Provide stability through implants • Add biologic stimulus when necessary
Infected Nonunions • Contaminated implants and devitalized implants must be removed • Infection treated: • Temporary stabilization (external fixation) • Culture specific antibiotics • +/- local antibiotic delivery (antibiobic beads) • Secondary stabilization with augmentation of osteogenesis (cancellous grafting)
24 year male with continued distal osteolysis after debridement, antibiotics and local beads
Once the infection Was resolved, bone Graft was applied and Healing ensued. Hardware removed and Infected bone debrided.
Persistent drainage And gross motion after Multiple attempts at Surgical treatment
Followed by proximal Corticotomy and Distraction to restore length Treatment consisted Of resection of Infected bone, acute Shortening and External fixation
Methods of Adding Stability • Cast/Brace – rarely sufficient in nonunions • External Fixation • Plates • Intramedullary Devices
Largest indication is a temporary stabilization following infection debridement Also useful in correction of stiff deformity and lengthening External Fixation
Plate Stabilization • Plates provide a powerful reduction tool • Surgical technique should strive for absolute stability • Locking plates have improved stability and fixation strength • Other relative indications: • Absent medullary canal • Metaphyseal nonunions • When open reduction or removal of prior implants is required
Multiple Indications for plate Broken implants require that removal Metaphyseal nonunion Significant deformity Technique Blade properly positioned in the distal fragment Reduction obtained by bringing plate to the shaft Absolute stability with lag screw Nonunion was not exposed Plate Stabilization Broken plate
Ideal case – Femur or tibia with an existing canal and no prior implants Exchange nailing provides a good option for the tibia and femur Special equipment is often necessary to traverse sclerotic canals Nail Stabilization
Adding Biology • Often unnecessary in hypertrophic cases with sufficient inherent biologic activity • Options • Aspirated stem cells (with or without expansion) • Demineralized Bone Matrix • Autogenous Cancellous Graft • Growth Factors • Platelet derived • Recombinant BMPs • Gene Therapy
Autogenous Cancellous Bone • Sites • Posterior Iliac Crest (20 cc) • Anterior Iliac Crest (10cc) • Proximal Tibia (7cc) • Distal Radius, Calcaneus, Olecronon (?) • All series suggest some incidence of donor morbidity dependent upon harvest site and volume required • Still considered by many to be the most osteogenic graft material
Demineralized Bone Matrix • Osteoinduction has been experimentally demonstrated* • Osteoinductive ability appears variable between products and donors • A consecutive series with historic controls has demonstrated effectiveness in humeral shaft nonunions • Avoids the morbidity of iliac crest graft • As effective as iliac crest ????? (doubtful in the authors opinion) *Hierholzer et al J Bone Joint Surg 2006
Aspirated iliac crest stem cells has been shown to enhance the activity of osteoconductive grafts Has been studied as an isolated technique with limited success Role of expansion and delayed implantation may play a future role Stem Cells
Recombinant Bone Morphogenic Proteins • BMP-2 • Infuse™ • Demonstrated effective in acute open tibial fractures • FDA approved in acute fractures • BMP-7 • OP-1™ • Comparable to autograft in tibia nonunions • FDA approved under HD exemption
BMP-2 for Open Tibial Fractures:Prospective & Randomized with 450 Patients • Results • High dose BMP-2 treatment led to 44% reduction in risk of nonunion/delayed union • Significantly fewer invasive interventions • Significantly faster fracture healing • Significantly fewer hardware failures and fewer infections BESTT Study Group, et al. J Bone Joint Surg 84A: 2123, 2002.
OP-1 in Tibial Nonunions • Prospective, randomized study • 122 patients with 124 tibial nonunions • Treatment • IM nail • 70 % exchange nail • 20 % new 1º nail • 10 % maintained prior nail • OP-1/collagen vs. ICBC • Clinical success: • 81% BMP7 • 85% ICBG Friedlaender GE et al, J Bone Joint Surg, 2001: 83A, Suppl 1; S1-151.
Improved understanding of BMPs Optimize BMP carriers Explore role of expanded stem cell lines Role of gene therapy Reduce the cost of production of inductive agents DNA coding for growth factor released growth factor from cell adenoviral vector carrying growth factor making ribosomes gene growth factors nucleus cell Ongoing Osteoinductive Research will likely change the future-
Osteoinduction Summary • The diversity and limited numbers of nonunions make Level 1 studies rare • Personal Opinion: • Nothing in hypertrophic or rodded nonunions • DBM in biologically friendly environments (humerus) • Autologous cancellous graft in challenging cases • BMP when ABG has failed or is not feasible
Specific Anatomic Sites • Clavicle • Humerus • Forearm • Femur • Tibia • Metaphyseal
Clavicle Nonunions • Middle 1/3 treated with compression plating +/- graft • Anterior or superior plate position • 95% union reported* • Lateral 1/3 treated with ORIF or excision and ligament reconstruction *Ballmer J Shoulder Elbow Surg 1998
HUMERAL NONUNION • 24 patients age 52-86yrs (ave 72yrs) • Locking compression plate with bone graft or DBM • All healed – 2 of the DBM cases needed secondary surgery for bone grafting • Ring et al, CORR 425, 2004
Recommended treatment is • rod removal and plating Humeral Failed Intramedullary Treatment • Avoid the temptation to • Perform exchange nailing • Union rates with exchange nailing • McKee 60% • Robinson 40% • Flinkkilla 46%
Forearm • Compression plating for hypertrophic nonunions • Critical attention to preservation of radial bow and radio-ulnar relationship • Cancellous graft for atrophic nonunion or bone loss
Forearm Nonunion with Bone Loss Grafted defect • 35 patients, both bones 8, ulna 11, radius 16 • All with segmental defects • Treatment • 3.5 plates, autologous cancellous bone graft • All nonunions healed • Improved function • Ring et al. JBJS 86A 2004
Dynamization failed to work Plating failed to work Revision plating Failed to work Primary surgery. A short Nail was chosen because of intertrochanteric fracture. Femoral nailing and Grafting has failed to work Femoral Nonunions • Low incidence with good primary surgery • Stabilization may be performed with either plate or rod • Despite the rarity, cases can become challenging as evidenced by this case