Download
1 / 81
840 likes | 1.22k Views
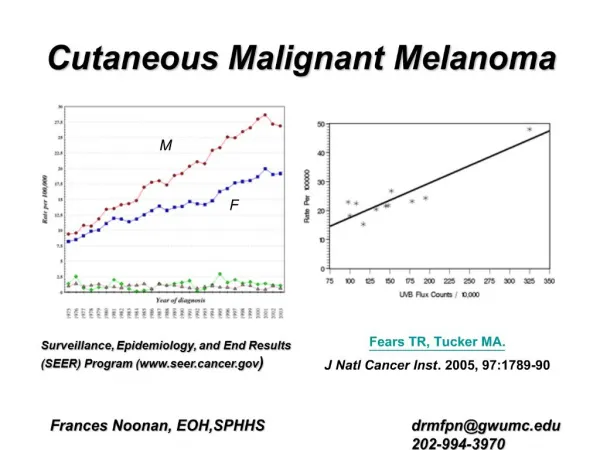
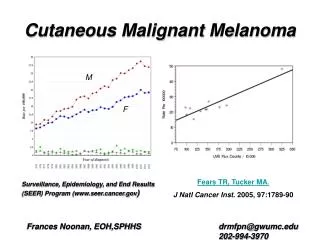
Cutaneous Head and Neck Melanoma. Melanoma is the fifth most common cancer in men, and the sixth in women in the United States25-35% will be found in the head and neckThe incidence has steadily increased over the past five decades (4.3% annual percentage change)It is highly curable when found at an early stage.

E N D
1. Cutaneous Head and Neck Melanoma Michael Briscoe Jr., MD
Vicente Resto, MD, PhD
University of Texas Medical Branch
Department of Otolaryngology
Grand Rounds Presentation
July 29, 2009
2. Cutaneous Head and Neck Melanoma Melanoma is the fifth most common cancer in men, and the sixth in women in the United States
25-35% will be found in the head and neck
The incidence has steadily increased over the past five decades (4.3% annual percentage change)
It is highly curable when found at an early stage
3. Cutaneous Melanoma Melanocytes reside in the basal layer of the epidermis.
They produce melanosomes which they share with adjacent keratinocytes through dendritic processes.
Melanoma is uncontrolled proliferation of melanocytes
4. Anatomy of the Skin
5. Etiology and Risk Factors The main risk factor for melanoma is sun exposure.
Intensity of exposure
Distance from equator
Age at exposure
History of sunburns
Sun block may provide false sense of security leading to prolonged sun exposure. (Autier 2007)
6. Other risk factors Hobbies or jobs that require prolonged sun exposure
Fitzpatrick types I-III
Red/blonde hair
Blue/green eyes
Freckles
> 100 in adults
> 50 in children
7. Genetic factors Estimated 5-12% of people diagnosed with melanoma have a family history of melanoma
4 genes have been isolated from families with increased incidence of melanoma
Cyclin-dependent kinase 4A (p16)
ARF (p14)
Cyclin-dependent kinase 4
melanocortin1 receptor
8. p16 Tumor suppressor gene found in 10-40% of melanoma prone families
Mutation to this tumor suppressor gene is found in virtually all melanomas
Important in cell cycle regulation during G1 checkpoint
Inhibits phosphorylation of retinoblastoma protein by CDK4.
9. MC1R Transmembrane receptor expressed in melanocytes.
Mediates melanin production after UV radiation or stimulation by hormones.
Protooncogene
Autosomal dominant, with low penetrance
10. Other genetic disorders Xeroderma pigmentosa
Multiple skin cancers
Decreased ability to repair DNA damaged by UV light
Increased susceptibility to melanoma
Congenital nevi
Present at birth
Those greater then 20 mm have a 5-10% chance of developing melanoma
11. Patterns of melanoma There may be horizontal growth that may take years to grow (superficial spreading)
Or there may be vertical growth
Vertical growth may take years
May occur rapidly (4 months � 2 years)
Melanoma in chronically exposed skin
Melanoma in intermittently exposed skin
12. Types of melanoma Lentigo maligna (Hutchinson freckle)
Lentigo malignant melanoma
Nodular
Desmoplastic
Mucosal
Multiple rare types
13. Lentigo maligna Melanoma in situ
Found in chronically sun exposed areas
Cheek > nose > forehead > ears > neck
60-70 year olds with no gender preference
Confined to epidermis
14. Lentigo malignant melanoma There is violation of basement membrane of epidermis into dermis
Spread is usually horizontal, followed by vertical spread
Irregular borders
7th decade
15. Nodular Rapidly enlarging nodule (4 months - 2 years) that is black, pink, or blue
Age 40-50, but can occur from 30-70s
0.4 � 5.0 centimeters with asymmetry and well defined borders
16. Desmoplastic Rare subtype with angiotropism and neurotropism
Locally aggressive and infiltrative
Characterized by spindle cells in desmoplastic stroma
17. Mucosal melanoma Clinically distinct from cutaneous melanoma
6th-7th decade
Black, brown, tan, pink, white, blue, or gray
Can be amelanotic
Poor prognosis
Most frequently found in the nasal cavity (anterior septum > inferior/middle turbinates) followed by oral cavity (hard palate and maxillary alveolar ridge).
18. Unusual variants of melanoma Amelonotic
Spindle cell
Small cell
Nevoid
Verrucous
Spitzoid
Balloon cell
Malignant blue nevus
19. Clinical Presentation Comprehensive history and physical examination
Targeted questions about sun exposure, hobby/job history
Family history of skin cancers
Previous skin cancers
Duration of lesions
Number of lesions
20. ABCDE Asymmetry
Borders
Variegated, or irregular borders
Color
Variegation of color, jet black, change in color
Diameter
Greater than 6 mm
Evolving
Bleeding, ulceration, pruritis to an old lesion
21. Additional Questions Constitutional symptoms
Pulmonary
Gastrointestinal
Hepatic
Musculoskeletal
Neurologic
Integumentary
22. Physical Exam Full head and neck exam
Inspection of the entire skin surface of head and neck as well as full body evaluation
In men, melanoma is most commonly found in the trunk/back followed by extremities, then head and neck region
In women, it is most commonly found in the extremities, followed by trunk/back, then head and neck
23. Differential Diagnosis Includes processes with melanocytic proliferation
Markedly atypical nevi
Halo nevi
Spitz tumors
Pigmented spindle cell tumors
Processes from sun damaged skin
Actinic keratosis
Solar lentigo
Solar melanocytic hyperplasia
Variety of pigmented sarcomas
Kaposi�s sarcoma
Angiosarcoma
leiomyosarcoma
Metastatic disease
SCCa
SCCa spindle cell variant
24. Diagnosis Requires full examination of skin
Biopsy of suspicious lesions
Avoid shave biopsy because they give no information on thickness of lesion
Excisional with 1-2 mm margin, full thickness punch biopsy, or full thickness incisional biopsy.
25. Histology Hematoxylin and eosin stain shows
Melanocytic proliferation, pleomorphism, high nuclear to cytoplasmic ratio, enlarged nuclei and nucleoli.
Pagetoid spread
Lentiginous melanocytic proliferation
Immunohistologic staining
S-100, HMB-45, vimentin, MART1
Cytokeratin negative
26. Histology
27. Clark Qualitative Levels All tumor cells within the epidermis, superficial to basement membrane
Tumor involves, but does not completely fill the papillary dermis
Tumor fills the interface between papillary and reticular dermis
Tumor cells invade the reticular dermis
Tumor involves subcutaneous tissue
28. Breslow Quantitative Stage < 0.75 mm
0.76 � 1.49 mm
1.50 � 3.99 mm
> 4.0 mm
29. Significance of Breslow and Clark levels Breslow depth has been correlated with prognosis
Clark levels are useful for differentiating lesions that are less than 1 mm in thickness (T1 lesions)
30. Other diagnostic tests FNA of suspicious lymph nodes
Radiographic
CXR
CT head, neck, abdomen, pelvis as indicated
MRI as indicated
Laboratory
Lactate dehydrogenase for distant metastasis
31. Cutaneous Melanoma Staging
32. Cutaneous Melanoma Staging
33. Cutaneous Melanoma staging
34. Cutaneous Melanoma Staging
35. Cutaneous Melanoma Staging
36. Cutaneous Melanoma Staging
39. Prognostic factors Thickness of primary lesion
Presence or absence of ulceration (histologic)
Number of metastatic lymph nodes
Presence or absence of In transit disease
Distant metastasis (skin, lung, visceral)
45. Definitive Treatment Wide local excision of melanoma
Depends on size of lesion
Melanoma in situ 0.5 cm margin
< 1.0 mm, then 1 cm margin
1.0 � 2.0 mm, then 1 � 2 cm margin
> 2.0 mm, then 2 cm margin
Sentinel lymph node biopsy
Therapeutic neck dissection
Reconstruction
46. Staged incision technique Moller et al retrospective chart review of 49 patients with lentigo maligna (melanoma in situ) of the head and neck.
Staged marginal and central incision technique
5 mm margin, then 2-3 mm marginal excisions
After negative margins (7-10 days), performed excision of central specimen with reconstruction Moller et al, Annals of Surgical Oncology, 2009
47. Staged Incision Moller et al, Annals of Surgical Oncology, 2009
48. Staged incision Kept incisions within aesthetic facial units
Reconstructed with FTSG, STSG, or rotational flaps
12% were upstaged to malignant melanoma
No recurrences with 14 month follow-up Moller et al, Annals of Surgical Oncology, 2009
49. Lymph node assessment in melanoma 90% of patients with melanoma have no evidence of lymphadenopathy on presentation
20% have occult neck disease
Elective neck dissection is no longer recommended due to morbidity of procedure
Morton was the first to use sentinel lymph node biopsy for melanoma in 1992.
50. Sentinel Lymph node biopsy Ideally performed after excisional biopsy and concurrent with definitive wide local excision
Radiocolloid is injected into four quadrants around the lesion 1-12hr prior to SLNB
Lymphoscintogram identifies areas of uptake
In the operating room, isosulfan blue is injected intradermally until a wheal forms. This forces the dye into the lymphatics McMasters et al Journal of surgical Oncology 2004;86:212-223
51. SLNB A gamma probe is used to identify �hotspots� and a 1-3cm incision is made over the area of maximum radioactivity
SLN has 3:1 ratio of radioactivity compared to background, and 10:1 ration when compared to non-sentinel node.
Sentinel node will have blue color from dye, or the afferent lymphatics leading to the node will be blue.
Nodal basin is carefully examined using the gamma probe, as more than one SLN may exist McMasters et al Journal of surgical Oncology 2004;86:212-223
52. SLNB It is important to continue dissection until the background count is less than 10% of the hottest node because metastases may be missed if the threshold is raised above 10%.
For head and neck sites, it is important to excise the primary and its isotope blush before using gamma probe, due to overlapping drainage pathways. McMasters et al Journal of surgical Oncology 2004;86:212-223
53. Definition of False Negative for SLNB McMasters et al Journal of surgical Oncology 2004;86:212-223
54. Successful SLNB in Head and Neck Region Requires knowledge of the head and neck by surgeon as well as nuclear medicine specialist.
Learning curve of 30 procedures for most head and neck surgeons
Two probe system (technetium and blue dye) increases the sensitivity of SLNB. McMasters et al Journal of surgical Oncology 2004;86:212-223
55. Lymphoscintigraphy
56. Sentinel Lymph Node Mapping in Head and Neck Melanomas Schmalbach et al University of Michigan (2003)
Retrospective cohort study with 80 patients
Mean follow-up of 25 months, minimum f/u of 1 year
All with cutaneous melanoma of head and neck and staged with SLNB
Tumor depth > 1.0 mm or
Tumor depth < 1.0 mm with poor prognostic variables
Ulceration
Extension to deep margin, or regression
Young age Schmalbach et al 2003
57. SLNM Reliability Patients underwent lymphoscintigraphy with Tc 99m sulfur colloid, intradermally in 4 quadrants. (2-4 hours prior to surgery)
Isosulfan blue intradermally in the OR.
1-3 cm incision made over area of increased radioactivity, or preauricular incision for parotid lymph nodes
LN evaluated with H&E staining, if this was negative, then would use S100, Melan-A, or HMB-45 Schmalbach et al 2003
58. SLNM Reliability SLN found in 96% of cases
74% in neck nodal basins and 24% in parotid basin
Of the parotid basin, 28/30 (93%) patients underwent successful SLNB
17.5% had lymph node positive metastasis treated with modified radical, superficial parotidectomy, or posterolateral neck dissection.
4.5 % false negative rate (3/66 negative SLNB went on to have regional failure)
These rates are comprable to SLNB in non-head and neck sites. Schmalbach et al 2003
59. Comparison of HNCM vs Melanoma at other sites (OMS) Agnese et al The Ohio State University (2007) performed study to assess outcome of cutaneous head and neck melanoma versus melanoma at other sites.
Total of 755 patients underwent SLNB
Tumor thickness > 1.0 mm
Tumor thickness < 1.0 mm with poor prognostic factors
Ulceration, regression, or Clark level IV or V involvement Agnese et al 2007
60. SLNB in HNCM 131/755 (17.4%) of melanomas found in the head and neck
Significantly more SLN�s in the head and neck group. Despite this, there was a lower percentage of positive nodes (9.2% vs. 16.0%)
No notable difference in local, regional, or distant recurrence between groups.
False negative rate 5.9% vs 4.4%, not significant
HNM do not have a poorer outcome than OMS Agnese et al 2007
61. Recurrence and Survival after SLNB Gomez-Rivera et al 2008 M.D. Anderson Cancer Center
Retrospective chart review of 113 patients with CHNM who underwent SLNB (1993-2004)
96% successful in finding SLN
Follow-up 34 months, with 28% recurrence
Same criteria as UM and OSU for performing SLNB Gomez-Rivera et al
62. Recurrence and survival 83 patients were part of a prospective study in which they underwent SLNB and neck dissection of the nodal basins (I-V, II-V, parotid, postauricular, and suboccipital)
The remaining patients underwent SLNB, and therapeutic neck dissection if SLN was positive. Gomez-Rivera et al
63. Recurrence Location face > scalp > neck
At least one SLN, median of 3
26% of SLN localized to non-predicted sites, especially lesions in the anterior scalp
32 (28%) patients developed recurrence
5/90 (5.5%) with negative SLNB, had recurrence Gomez-Rivera et al
64. Survival 5 year DFS was negatively affected by female sex, Breslow thickness 2-4 mm, Clark level IV or higher, and positive SLN
5 year OS was negatively affected by age greater than 60, Breslow 2-4 mm, Clark level IV, and positive SLN
Concluded that tumor thickness and age were important factors in survival. (+) SLN showed a trend in intermediate thickness tumors for worse survival. Gomez-Rivera et al
65. Treatment of the Neck SLNB should be performed if there is no palpable nodal metastasis and the following criteria are met:
> 1.0 mm thicknes
< 1.0 mm thickness with poor prognostic factors
Ulceration
Clark level IV or V involvement
Significant regression of tumor
66. Treatment of the Neck Therapeutic neck dissection is carried out when there is positive nodal disease. This can be palpable, or node positivity from SLNB
Levels of neck dissection depend on location of melanoma, but modified radical or selective neck dissection is preferred
May need to dissect postauricular, suboccipital, or parotid nodes (superficial parotidectomy)
67. Treatment of Neck based on location of melanoma Face
Forehead
Auricle
Anterior scalp
Posterior scalp
68. Adjunctive therapy Interferon alpha-2b is the only FDA approved agent for therapy in high-risk patients (stage IIb and III).
The largest group of high risk patients are those with nodal metastasis.
Eastern Cooperative Oncology Group (ECOG) has had two trials which show disease free survival benefit with high dose interferon alpha-2b.
69. Adjunctive Therapy ECOG trial E1694 looked at interferon alpha-2b compared to ganglioside vaccine.
Interferon had increased DFS and OS compared to vaccine
All of these trials were in patients with bulky neck disease
Sunbelt Melanoma Trial is looking at the role of adjunctive therapy in patients with intermediate disease, and micrometastasis to lymph nodes.
70. Adjuvant Interferon therapy
71. Pegylated IFN-alpha 2b Eggermont et al (2008) conducted a randomized phase III study comparing the pegylated IFN-alpha 2b to observation in stage III melanoma (EORTC 18991)
1256 patients (629 obs, 627 IFN)
Median treatment length was 12 months
Median follow-up 3.8 years
Found improved RFS, but no change in OS
Pegylated IFN offers less side effects (toxicity), and has benefit beyond the treatment duration.
Best results in those with micrometastasis Eggermont et al, Lancet Vol 372
72. Radiation Therapy Reserved for stage IV disease, or disease with significant poor prognostic factors
Neurotropism
Greater than 4 node metastasis
Extracapsular spread
Recurrence
Phase III clinical trial is on-going
73. Chemotherapy Melanoma is relatively chemoresistant
Dacarbazine (DTIC) is the only approved agent
Only 10-20% of people have a response and less than 5% of people have a complete response
Reserved for Stage IV disease
74. Future Study There are a number of research protocols underway.
Management of intermediate disease, and micrometastasis will benefit from randomized control trials
Immunotherapeutic agents
75. Immunotherapy IL-2 is the only FDA approved cytokine for stage IV melanoma. 8 clinical trials have shown a 16% overall response rate, and 6% complete response
IL-21 currently being investigated in phase I and II clinical trials
Adoptive immunity � ex vivo activation and expansion of tumor-reactive lymphocytes taken from host, then reinfused into the patient
Human igG monoclonal antibodies
Iplimumab
tremelimumab
Eggermont AM and Schadendorf D, Hematol Oncol Clin N Am 23 (2009)
76. Immunotherapy Vaccines
Autologous
Allogeneic
MAGE-3 (RCT stage IIIB and IIIC planned)
Peptide based (ECOG 4697)
Dendritic cell based (inconclusive data)
Intratumoral gene transfer (Phase III trial planned) Eggermont AM and Schadendorf D, Hematol Oncol Clin N Am 23 (2009)
77. Summary Melanoma is the 5th and 6th most common causes of cancer in men, women in the United States
It is highly curable at an early stage (85-90%)
There are no good treatment options for late stage disease (Stage IV)
78. Summary The most important prognostic factors for intermediate melanomas are tumor thickness, presence of ulceration, and lymph node status.
Sentinel lymph node biopsy is an important part of nodal staging to find micrometastasis
Positive lymph node status upgrades to a stage III cancer (regional disease)
79. Summary Therapy remains wide local excision with margins for stages I - III, with the addition of neck dissection for stage III melanomas.
Adjunctive therapy is available, but more trials are needed to discover more effective treatments for stage III and IV disease.
80. Bibliography Agnese DM, Maupin R, Tilman B et al. Head and neck melanoma in the sentinel lymph node era. Arch Otolaryngol Head Neck Surg 2007,133(11):1121-1124
Autier P, Dore JF, Schifflers E, et al. Melanoma and use of sunscreens: an EORTC case-control study in Germany Belgium, and France. Int J Cancer 1995;61:749.
Autier P, Boniol M, Dore JF. Sunscreen use and increased duration of intentional sun exposure: still a burning issue. Int J Cancer 2007;121:1�5.
Balch CM et al. New TNM melanoma staging system: linking biology and natural history to Clinical outcomes. Seminars in Surg. Oncology 2003,21:43-52
Barnhill RL, Mihm MC, and Elgart G. Malignant Melanoma. Skin Cancer 1st ed 2008, Nouri K
Bottomley A et al. Adjuvant therapy with pegylated interferon alpha-2b versus observation in resected stage III melanomas: a phase III randomized control trial of health-related quality of life and symptoms by the European Organisation for Research and Treatment of Melanoma Cancer Group. J Clin Oncol 27:2916-2923
Doting EH, De Vries M, and Plukker J et al. Does Sentinel Lymph Node Biopsy in cutaneous Head and neck melanoma alter disease outcome. Journal of Surgical Oncology 2006,93:564-570
Easson AM, Rotstein LE and McReady DR. Lymph node assessment in melanoma. Journ of Surg Oncology 2009,99:176-185
Eggermont AMM. Melanoma and Immunotherapy. Hematol Oncol Clin N AM 2009:547-564
Eggermont AMM et al. Adjuvant therapy with pegylated interferon alpha-2b versus observation Alone in resected stage III melanoma: final results of EORTC 18991, a randomized phase III trial. The Lancet July 2008,372:117-126
81. Bibliography Gomez-Rivera F, Santillan A, McMurphey AB et al. Sentinel lymph node biopsy in patients with cutaneous melanoma of the head and neck: recurrence and survival study. Head And Neck Oct 2008,1284-1293
Gillenwater, AM and Harrison LB ed. Ch 22 Melanoma of the Head and Neck. Head and Neck Cancer: A Multidisciplinary Approach. 3rd edition, 2009
Lin D, Franc BL, Kashani-Sabet M, amd Singer MI. Lymphatic drainage patterns of head and neck cutaneous melanoma observed on lymphoscintigraphy and sentinel lymph node biopsy. Head and Neck March 2006,249-255
McDermott et al. Double Blind Randomized Phase II study of the Combination of Sorafenib and Dacarbazine in patients with advanced melanoma/; A report from the 11715 Study Group J Clin Oncol 26:2178-2185
McMasters KM et al. Lessons learned from Sunbelt Melanoma Trial. Journ of Surg Oncology 2004,86:212-223.
Tanis PJ, Nieweg OE et al. Dilemma of clinically node-negative head and neck melanoma: Outcome of �watch and wait� policy, elective lymph node dissection and sentinel lymph Node biopsy- A Systemic Review. Head and Neck March 2008:380-389
Schmalbach CE, Nussenbaum B, Rees RS et al. Reliability of sentinel lymph node mapping with biopsy for head and neck cutaneous melanoma. Arch Otolaryngol Head and Neck Surgery Jan 2003,129:61-65
Schmalbach CE, Johnson TM, and Bradford CR. Ch. 23 The Management of Head and Neck Melanoma. Cummings: Otolaryngology Head and Neck Surgery, 4th ed., 2005
Wolf P, Donawho CK, Kripke ML. Effect of suncreens on UV radiation-induced enhancement of melanoma growth in mice. J Natl Cancer Inst 1994;86:99�105.
82. Thank you