Download
1 / 20
200 likes | 380 Views
IMPROVING THE USE OF ARTEMISININ-BASED COMBINATION THERAPY IN RURAL ZAMBIA. Kojo Yeboah-Antwi Centre for Global Health and Development Boston University. Third International Conference for Improving Use of Medicines Antalya, Turkey November 15, 2011. Background .

E N D
IMPROVING THE USE OF ARTEMISININ-BASED COMBINATION THERAPY IN RURAL ZAMBIA Kojo Yeboah-Antwi Centre for Global Health and Development Boston University Third International Conference for Improving Use of Medicines Antalya, Turkey November 15, 2011
Background • Many sick children in rural Zambia are seen by community health workers (CHW) because public health facility-based services are not readily accessible • Zambia has changed first line drug for uncomplicated malaria to more expensive and effective artemisinin-based combination therapies (ACTs) • Relatively little known about how to optimally deploy ACTs to the community level • Concerns about potential overuse of ACTs and development of resistance if use by CHWs is not guided by rapid diagnostic tests (RDTs)
Overall Study Goal Demonstrate the effectiveness and feasibility of using CHWs to manage malaria (with artemether- lumefantrine) guided by RDTs
Objectives • Will RDT use lead to reduction of overuse of ACTs? • How well will CHWs follow a treatment algorithm and adhere to results of the RDTs? • Will children and CHWs experience any side effects with the pricking? • What happens to children with RDT negative results who do not receive ACTs? • Will the community accept CHWs performing RDTs and prescribing ACTs?
Southern Province of Zambia Mazabuka and Siavonga districts Chikankata Mission Hospital area Population: 70,000 1 Mission Hospital and 5 Rural Health Centers Study Location
Study Sites Hamukombwe CHP Chaanga RHC Mwanamunzya CHP
Study Design Cluster randomized, controlled trial around community health posts manned by CHWs Community health posts matched according to distance from rural health center
Intervention • Both intervention and control CHWs trained in classification and treatment of febrile illness • Both CHWs supplied with ACTs and antipyretics • Intervention CHWs received additional training on RDTs and infection control • Intervention CHWs received RDTs and supplies for waste disposal and infection control
Enrolment • Children aged 6 mo to 5 yrs with fever were enrolled • Children with severe illness excluded and referred • History, examination, RDT (in intervention arm), classification and treatment • Baseline form completed (findings, results, treatment, address)
Follow-up • Patients seen at day 5-7 to collect information on visit, outcome of treatment, additional care received • Determine current condition and advise as necessary • Monthly data from CHPs on patient seen, supplies and referrals • Post intervention FGDs and IDIs of caregivers, CHWs, health workers and community leaders
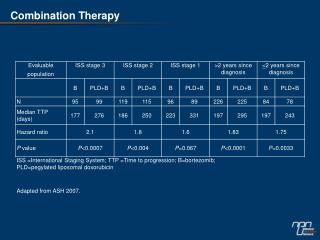
Results 1Intervention: classify as malaria if RDT (+), and not malaria if RDT (-)Control: classify as malaria if fever (+), and no malaria if fever (-) 2Prescribe ACT if classified as malaria; ACT not prescribed if classified as not malaria
Results • 975 RDTs done of which 271 (27.8%) were positive and 704 were negative • 3 of 704 RDT negatives received ACTs from CHWs • 4 of 271 RDT positives did not receive ACT from the CHWs • 5 of the RDT negatives who did not receive ACTs from CHWs were not satisfied and managed to get ACTs from other sources • 91.2% of the RDT negatives got well with only antipyretics and needed no additional treatment
Adverse Effects with RDT • Of 975 RDTs done: • 3 children with minor bruises • 2 children with skin infection • 14 children with minor bleeding • 1 incident of self prick
Community Acceptance • Caregivers were comfortable with CHWs pricking children to test for malaria • Caregivers trusted results of the RDTs • CHWs felt confident in performing RDTs and treating with ACTs • Health workers endorse CHWs use of RDTs and ACTs • Community leaders happy with intervention and want expansion to other areas and adults
Conclusions • CHWs are capable of performing RDTs and appropriately dispensing ACTs • Use of RDTs and ACTs by CHW is safe and effective • Use of RDTs at the community level by CHWs has potential to reduce the overuse of ACTs and improve ACT use • Health workers see CHWs involvement in malaria treatment with RDTs and ACTs as positive and has the potential to reduce workload at health facilities • Community acceptance of malaria treatment by CHWs is overwhelmingly encouraging
Limitations • More CHP attendance in Control arm resulted in relative imbalance between the two study arms • “full time” CHWs • Varied cluster size • No evidence of “contamination” • Recall bias • Designed not to repeat parasitological test at follow up
Study Team Kojo Yeboah-Antwi PortipherPilingana KazunguSiazelee William B. MacLeod Katherine Semrau Penelope Kalesha BusikuHamainza Donald Thea • Davidson H. Hamer • Lora L. Sabin • Karen Kamholz • EuphasiaMtonga • PascalinaChanda • Arthur Mazimba • Phil Seidenberg
Funding USAID/Washington through CFAR Cooperative Agreement GHSA-00-00020 with BU President’s Malaria Initiative (Washington DC)