Download
1 / 29
310 likes | 435 Views
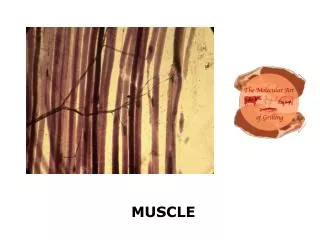
MYOTONIC MUSCLE DISORDERS. By Radwa ElKhouly Assistant lecturer of Physical Medicine and Rheumatology Tanta university. The myotonic muscle disorders and periodic paralysis syndromes.

E N D
MYOTONIC MUSCLE DISORDERS By Radwa ElKhouly Assistant lecturer of Physical Medicine and Rheumatology Tanta university
The myotonic muscle disorders and periodic paralysis syndromes • a group of disorders characterized by muscle stiffness, pain, and sometimes weakness, which may be intermittent or constant. • Myotonia is a phenomena of delayed relaxation after forceful voluntary contraction • Is due to repetitive depolarization of the muscle membrane
Myotoniasdisorders of muscle membrane excitability painless muscle stiffness Chloride channelopathies (CLCN1) – myotonia congenita (MC) autosomal dominant (Thomsen) 1876 autosomal recessive (Becker) 1977 – myotonic dystrophy type 1 and 2 Sodium channelopathies (SCN4A) • paramyotonia congenita (PMC) • SodiumChannelMyotoniaCongenita or potassium-aggravated myotonia (PAM) • hyperkalemic periodic paralysis (HyperPP)
Myotonic dystrophy type 1 (DMl) • T he most common; • Age at onset late teens • Inheritance autosomal dominant • Gene defect is due to a defect in the protein kinase myotonia gene on chromosome 19q
Myotonia Distribution • The myotonia mainly distal demonstrated with grip and percussion myotonia can be elicited most easily over the thenar muscles and long finger extensors. • Mild weakness &wasting distal & bifacial, neck flexor ms the distal › proximal, • Ms stiffness that improves with repeated contractions.
There is a characteristic clinical appearance • Bifacialweakness • Temporal wasting • Frontal balding, resulting in a narrow, elongated face and horizontal smile • ptosis, • Eyelid myotonia is not seen. • Deep tendon reflexes often are reduced or absent in the lower extremities as the disease progresses.
Extra muscular involvement • Cataracts, Slitlamp examination reveals posterior capsular cataracts, which early on have a characteristic multicolored pattern. • Cardiac Conduction defect as arythmia • Pulmonary Defects excessive daytime sleepiness due to weakness of the diaphragm and intercostal ms • Endocrine Dysfunction, insulin resistance • Testicular Atrophy, • Gynecologic Problems, • In Some Patients, Mild To Moderate Cognitive Impairment. • Provocative Factors :None • Alleviating Factors: None
Congenital: • Approximately 10%, • characterized by severe weakness and hypotonia at birth • mental retardation. • maternally inherited. In many cases, the mother may be so minimally affected that her diagnosis is not made until the infant is born with severe hypotonia and a myopathicfacies. Laboratory: • Creatinekinase (CK) levels may be mildly to moderately elevated. Muscle biopsy: typically reveals atrophy of type I muscle fibers, increase in central nuclei, ring fibers, and occasional small angulated fibers
Myotonic Dystrophy Type 2 • Age at onset: Teens to early adult • Inheritance it is an autosomal dominant • Gene defect: Zinc finger protein-9, chromosome 3q
MyotoniaDistribution: • myotonia, in the setting of grip and percussion myotonia. • Including bifacial weakness, ptosis, progressive weakness, • predominantly proximal, although proximal and distal weakness is seen, • And some patients may have muscle hypertrophy. • Frontal balding
Extra muscular involvement : • Posterior capsular cataracts, • Testicular atrophy, and • Cardiac conduction defects. • Many patients have an intermittent pain syndrome in the thighs, arms, or back. • Provocative Factors :None • Alleviating Factors: None • Laboratory: • Ck may be mildly to moderately elevated, The muscle biopsy reveals a nonspecific myopathic pattern, including variation in fiber size, hypertrophy of type ii fibers, and increased central nuclei.
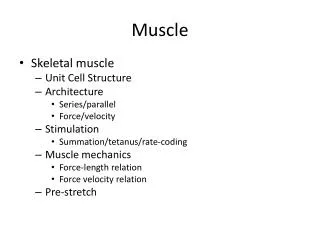
Andersen Syndrome in childhood or adolescence, with some or all features of the clinical triad of • periodic paralysis • ventricular arrhythmias & Prolonged QT interval • dysmorphic facial features. include short stature, high arched palate, low-set ears, broad nose, micrognathia, short index finger, and syndactyly of the toes Scoliosis may be present. generalized limb and neck flexor weakness. no grip or percussion myotonia. Paralytic attacks may occur spontaneously or may be triggered by rest after exercise or alcohol. May intermittent muscle pain without attacks of weakness
Characteristic facial features in Andersen syndrome. Note low-set ears. broad nose,.
Schwartz-Jam pel Syndrome • characterized by skeletal deformities, muscle stiffness, and myotonia. • distal weakness and atrophy, with proximal upper and lower extremity muscle hypertrophy. • Characteristic facial and physical appearance include short stature, short neck, and multiple facial anomalies (micrognathia, low-set ears,pursed lips, prominent eyebrows, upward slanting eyes,blepharophimosis, exotropia, and microcornea) • 20% with cognitive impairment.
EMG in myotonia • Routine motor and sensory nerve conduction one or two motor and sensory conduction studies and corresponding F responses in an upper and lower extremity. Distal CMAPs may be low in the dystrophic myopathies.
2. Needle EMG proximal and distal muscles of one upper and lower extremity, as well as facial and paraspinal muscles. • abnormal spontaneous activity, including myotonic discharges, complex repetitive discharges, fibrillation potentials and positive waves • MUAPlow amp, short duration and polyphasic
A myotonic discharge: • The spontaneous discharge of a muscle fiber • Waxes and wanes in both amplitude and frequency. • Myotonic potential may have either a positive wave or a brief spike morphology. • Produce a divebomber sound on emg.
3. Muscle cooling : paramyotoniacongenita. • A. Wrap the limb in a plastic bag, submerge in ice water for about 10 to 20 minutes to bring skin temperature to 20· • C. Remove the patient's hand from water. • B. Needle EMG of a distal forearm or hand muscle is performed, noting the presence of abnormal spontaneous activity (fibrillation potentials, myotonic bursts)
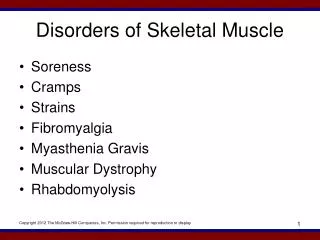
4. Short exercise test. • . Record at abductor digitiminimi stimulating ulnar nerve at the wrist. • B. Record the CMAP once per minute for 5 minutes with muscle at rest to ensure no decrease in the baseline CMAP. • C. maximum voluntary contraction for 5 to 10 seconds. • D. Record the CMAP immediately. If a decrement in amplitude is seen, continue to record the CMAP every 10 seconds until it recovers to baseline (typically 1-2 minutes).
a brief maximal voluntary contraction, the compound muscle action potential (CMAP) immediately decrements in the myotonic syndromes. If subsequent CMAPs are evoked every 10 seconds, the decrement recovers to baseline in 1 to 2 minutes in myotonic dystrophy and myotonia congenita (top), Numbers on the left refer to the time in seconds measured after the exercise. In paramyotonia congenita, the recovery may be quite delayed, in the range from 10 to 60 minutes.
5. Prolonged exercise: • a. Have the patient perform maximal voluntary muscle contraction for 2 to 5 minutes, resting every 15 seconds for 3 to 4 seconds. then relax completely. • c. Record the CMAP immediately, then every 1 to 2 minutes for 40 to 60 minutes afterward or until there is no further decline observed in the CMAP. • Decrement is calculated as follows: (Highest CMAP amplitude after exercise - Smallest CMAP amplitude after exercise)/(Highest CMAP amplitude after exercise x 100). Any decrement >40% abnormal.