Download
1 / 48
490 likes | 670 Views
Practical Evaluation of a Pharmacoeconomic Paper. Dr J Miot Wits University May 2011. What is “Health”?. World Health Organisation: Health is a “state of complete physical, mental and social well-being”. Everyone wants it!. HEA PTP: M207 Health Economics. Why do we need Health Economics?.

E N D
Practical Evaluation of a Pharmacoeconomic Paper Dr J Miot Wits University May 2011
What is “Health”? World Health Organisation: Health is a “state of complete physical, mental and social well-being” Everyone wants it! HEA PTP: M207 Health Economics
Why do we need Health Economics? • “All effective health technologies should be free” • Archie Cochrane • But • The introduction of new effective technology is faster than the increase in our ability to pay for them • Uncertainty about both effects and resource use for new technologies
Economic Drivers of Healthcare Costs • Increasing population • Changing population • Increase in pace and price of new technology • Patient choice and expectation • Economies of scale (pvt vs public) • Tensions between different fund options • Lack of legislative bodies to control price and quality of new health treatments • Role of country’s economic well being
Its all about choices • Resources are scarce • What we “want” is unlimited • Therefore involves “choice” • How do we choose? HEA PTP: M207 Health Economics
Balancing Uncertainty and Access • Unrestricted Access • Spending scarce healthcare resources on technologies that provide little if any benefit or may even harm • Restricted Access • Delaying benefits which could be accrued whilst generating further evidence on effectiveness • Need to explore ways to take into account uncertainty while also offering chance for earlier/increased access to novel treatments Trueman P. ISPOR SA 3rd Annual Conference 2010
Health Economics and Choices • “Assessment of the overall value of a healthcare intervention for the allocation of resources in a given environment” • Maximise the benefits from available resources • Provides tools to make consistent decisions • Provides value for money based on cost-effectiveness and not on the basis of cost alone
Uses of Health Economics Studies • Submission for Re-imbursement • Submission for Regulatory approval • Academic and Educational • Publication for information • National Guidance • Policy Determination • Cost-Benefit Analysis
Lets start with an example.... • This workshop is giving you a headache! You need treatment for immediate relief. • Your treatment options are: • Which is the most cost-effective option?
Which is the most cost-effective option? • What do you look at first? • Clinical Evidence! • Which products have proven clinical benefits? • Are they all the same or are there differences in outcome? • Paracetamol = ibuprofen > tramadol • Now look at the costs • Which is the most cost-effective option? • Sachs C. Oral analgesics for acute non-specific pain. Am Fam Physician 2005;71:913-18.
What are the costs.... • The costs for your treatment options are: • Which is the most cost-effective option?
What are the components of Health Economics? • The COMPARATIVE analysis of alternate treatments in terms of COSTS and CONSEQUENCES ( can be more than one alternative). Drug Consequences A A CHOICE Costs A B Consequences B Costs B Comparator
Incremental benefits and costs Generally going to spend more money so have to ask “Is the increased benefit worth the increased cost?” Incremental Cost Effectiveness Ratio = (Costs B – Costs A) ICER (Effects B- Effects A)
The Cost-effectiveness Plane More Costly Weak Moderate TX is less effective and more costly Upper Threshold Lower Threshold DOMINANT Strong More Benefit Less Benefit Weak Lower Threshold TX is more effective and less costly Upper Threshold Moderate DOMINANT Strong Less Costly
Part of a Decision-making Process Clinical Evidence Epidemiology Financial Costs Health Economics Patient Access Budget Impact Communication and Implementation
Type of HE Study Design: Cost Minimisation Analysis (CMA) Cost Effectiveness Analysis (CEA) • Same outcome, different costs • e.g. antibiotics, generics • “the cheapest option” • Different outcome, different costs • Usually measured in events prevented, lives saved • e.g. Open vs. laparoscopic surgery Cost Utility Analysis (CUA) Cost Benefit Analysis (CBA) • Multiple outcomes, different costs • ‘soft’ measures - pain, suffering and disability • ‘hard’ measures - years of reduced life, restenosis • Combined into a single outcome measure: Quality Adjusted Life Year (QALY) • e.g. biologics in Rheumatoid Arthritis • Similar to CUA but the output measure expressed in monetary units. • Measured in terms of “Willingness to pay” • e.g. cost of diabetic counselling
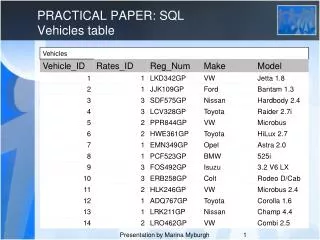
Cost Minimisation Analysis 255.62 402.09 Forcid Tavaloxx 500 224.45 268.56 • Meta-analysis flouroquinolones vs beta-lactam antibiotics in acute bacterial sinusitis. OR 1.09 (0.85-1.39) • Canadian Medical Association Journal 2008;178(7):845-854 • Bradley J et al. NEJM, 1991;325(2):87-91
Cost-minimisation analysis 381.43 288.54 726.88 Now add: GP consult R211.30 – R332.00 And maybe even; CT Sinus R534 – R3044 MRI Sinus R4474 – R7171
Type of HE Study Design: Cost Minimisation Analysis (CMA) Cost Effectiveness Analysis (CEA) • Different outcome, different costs • Usually measured in events prevented, lives saved • e.g. Open vs. laparoscopic surgery Cost Utility Analysis (CUA) Cost Benefit Analysis (CBA)
Cost-effectiveness Analysis What is the ICER? (C1-C2)/(E1-E2) Cost/Lives saved = (10 000 – 2 000)/ (0.07 – 0.1) = R266 666/additional deaths prevented
Type of HE Study Design: Cost Minimisation Analysis (CMA) Cost Effectiveness Analysis (CEA) Cost Utility Analysis (CUA) Cost Benefit Analysis (CBA) • Multiple outcomes, different costs • ‘soft’ measures - pain, suffering and disability • ‘hard’ measures - years of reduced life, restenosis • Combined into a single outcome measure: Quality Adjusted Life Year (QALY) • e.g. biologics in Rheumatoid Arthritis
Quality Adjusted Life Years (QALYs) • QALYs are generally considered the standard unit of comparison for measuring quality of life outcomes in health economic evaluations • QALYs = time (years) x quality (utilities) • e.g after amputation above the knee – LE is 40 years but utility is 0.875 • 40 x 0.875 = 35 QALYs
Years of Life at Full Quality Utility Years of Life
Loss of years and quality of life Reduced Quality of Life Catastrophic illness starts Utility Reduced Years of Life Years of Life
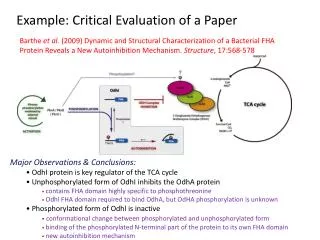
Current Treatment A • 1 QALY’s* gained with • 0.9 treatment A = 3.5 Cost: R200,000 • 0.8 • Improved Quality of Life • 0.7 No treatment • 0.6 0.5 Utility • 0.4 • 0.3 • Improved Years • 0.2 • 0.1 • 0 • 0 • 1 • 2 • 3 • 4 • 5 • 6 • 7 • 8 • 9 Years of Life Improved Quality of Life Improved Years of Life • *Quality Adjusted Life Year
New Treatment B • 1 QALY’s* gained with • 0.9 treatment B = 3.65 Cost: R290,000 Improved Quality of Life • 0.8 • 0.7 No treatment • 0.6 • 0.5 • Utility • 0.4 • 0.3 Improved Years of Life • 0.2 • 0.1 • 0 • 0 • 1 • 2 • 3 • 4 • 5 • 6 • 7 • 8 • 9 • Years of Life • *Quality Adjusted Life Year
1 1 1 1 QALY QALY ’ ’ s s * gained with * gained with QALY QALY ’ ’ s s * gained with * gained with 0.9 0.9 0.9 0.9 treatment B = 3.65 treatment B = 3.65 treatment A = 3.5 treatment A = 3.5 Cost: R290,000 Cost: R290,000 0.8 0.8 0.8 0.8 Cost: R200,000 Cost: R200,000 Improved Improved 0.7 0.7 0.7 0.7 No treatment No treatment No treatment No treatment Quality of Life Quality of Life 0.6 0.6 0.6 0.6 0.5 0.5 0.5 0.5 Utility Utility 0.4 0.4 0.4 0.4 0.3 0.3 0.3 0.3 Improved Improved 0.2 0.2 0.2 0.2 Years of Life Years of Life 0.1 0.1 0.1 0.1 0 0 0 0 0 0 1 1 2 2 3 3 4 4 5 5 6 6 7 7 8 8 9 9 0 0 1 1 2 2 3 3 4 4 5 5 6 6 7 7 8 8 9 9 Years of Life Years of Life Years of Life Years of Life Choice of Treatment: Treatment A = R200,000 per 3.5 QALY’s* Treatment B = R290,000 per 3.65 QALY’s* Incremental Cost-Effectiveness Ratio = (290,000-200,000)/(3.65-3.5) Incremental Cost/QALY* = R600,000/QALY* *Quality Adjusted Life Year
Is it a health economics study? • Comparison of two or more alternatives? • M. Drummond et al, Methods for Economic Evaluation of Health Care Programmes. 2nd Ed. 1997
Steps to Evaluating Health Economics • 1. What is the question being answered? • Was a well-defined question posed in answerable form • Look in the introduction and methodology for this info Drummond et al, 1996. Methods for the Economic Evaluation of Health Care Programmes. Chap 3.
2. Are these results useful to me in my setting? • Only if methodology is appropriate and results are valid • Not every study will answer every question • Will reveal weaknesses and strengths of the study
Study Perspective • Societal : all costs and outcomes • Third party payer : public or private • Health care provider : hospital • Benefits manager in private industry : direct medical costs to employees, productivity of employee • Patients : out of pocket expenses, travel and waiting time
Time horizon • Depends on the intervention and the associated harm or benefit • Days • Weeks • Months • Years • Lifetime
3. What are the Clinical Comparators? • Are they properly described? • Were any important alternatives omitted? • Was (should) a do-nothing alternative be considered? • Was an appropriate alternative chosen?
4. Is there evidence of effectiveness? • Is it from randomized clinical trials, meta-analysis or expert opinion? • Is it effective in clinical practice? • Were observational data or assumptions used to establish effectiveness? What about potential biases? • Is the appropriate patient population being evaluated? • If the treatment is not safe or effective – don’t go any further!
5. What are the Clinical Measures? • Hard endpoints – survival, events, cures • Surrogate markers – BP, TC, Viral load etc • Are they relevant and appropriate? • How are they presented? OR, RRR, AR etc
6. What costs were measured? • Depends on Perspective • Direct medical costs: drug acquisition costs, pharmacy dispensing costs, lab costs, physician visits for monitoring, treatment of side-effects etc • Indirect cost: decreased productivity, absenteeism, income lost, forgone leisure time, time spent by pt seeking medical services, time spent by family and friends attending the pt • Intangible cost: psychosocial costs, apprehension, anxiety, grief, loss of well-being, social isolation, family conflict, pain, changes in social functioning and activities of daily living
What costs were measured? • Cost = price x utilisation • Were the costs measured correctly in appropriate physical units • What measures were used? Were they appropriate? • What was omitted from measurement – why? • Any special circumstances that make measurement difficult?
Were the costs and consequences adjusted for differential timing • Were costs and outcomes occurring in the future “discounted” to present value • Was there any justification of discount rate used? • Were all cost brought to a fixed time period?
7. What are the Health Economic Measures? • Was an incremental analysis performed? • Incremental Cost/Life year gained (LYG) • Incremental Cost/QALY • Incremental Cost/event prevented • Incremental Cost/procedure
8. How confident are you that this is a valid outcome? • Was a sensitivity analysis performed? • Was justification provided for the range of values? • Which parameters were sensitive to change and reasons given for why? • Has a statistical analysis been done?
9. Presentation and Discussion • Did the presentation and discussion of study results include all issues of concern to users? • Interpreted intelligently or mechanistically? • Results compared with other similar studies? What were differences/similarities • Discussion on generalisability of results to other settings or pt groups? • Account for other important factors? • Discuss impact and feasibility of implementation? • Conflict of Interests?
What is your perspective? Pessimist: bottle ½ empty Optimist: bottle ½ full Economist: bottle ½ wasted inefficient! HEA PTP: M207 Health Economics
Challenges in HE Analysis • Lack of direct comparisons to relevant alternative • Head-to-head trials often not available • Comparator in trials may not be relevant in our setting • Measuring relevant costs and benefits • Vary from country to country ( transferability) • Value of surrogate endpoints • Lack of long-term follow-up – extrapolation beyond clinical trials • Especially important in chronic disease • Some modelling is required • Decision needed now - can’t wait until long-term data is available • Relevance to local settings – adapting from other settings • Local costs and resource utilisation • Reducing uncertainty to improve confidence in outcome • Sensitivity analysis • Cost-effectiveness acceptability curves plotted from probabilistic models
Challenges are Opportunities • Using EBM and Health Economics leads to; • Better clinical outcomes • More efficient use of resources • Reduce over-utilisation • Reduce perverse incentives • Improved re-imbursement structures • Improved training and skills
What Levels of Training are needed? • Education and Skills needed to conduct, interpret and use economic evaluations in healthcare. ISPOR Panel 4. Value in Health, 1999. 2 (2):88-91
Websites and other useful info • ISPOR www.ispor.org • NICE www.nice.org.uk • Cochrane Database • http://www.healtheconomics.com/ • Guidelines for authors and peer reviewers of economic submissions to the BMJ. Drummond M and Jefferson TO. BMJ, 1996:313:275-283 - Notes in file • Challenges in systematic reviews of economic analyses. Pignone et al. Ann Intern Med, 2005:142:1073-1079 • Methods for Economic Evaluation of Health Care Programmes. Second Edition. Drummond et al. Oxford Medical Publications