Download
1 / 37
440 likes | 890 Views
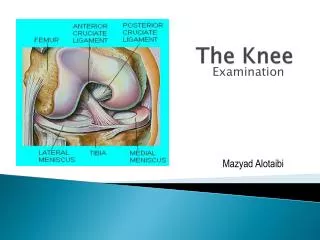
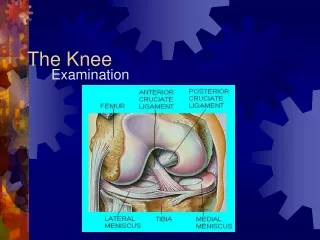
Chapter 21 The Knee. Anatomy. Subdivisions of Synovial Cavity. Anterior Rectus femoris Vastus lateralis Vastus intermedius Vastus medialis Medially Gracilis Adductor longus, brevis, magnus. Posterior Biceps femoris Semitendinosus Semimembranosus Laterally

E N D
Anterior Rectus femoris Vastus lateralis Vastus intermedius Vastus medialis Medially Gracilis Adductor longus, brevis, magnus Posterior Biceps femoris Semitendinosus Semimembranosus Laterally TFL/ITB (affected by gluteus maximus, etc.) Myology
Kinematics – Tibiofemoral Joint ROM Flexion/extension 0-140 degrees Extension– Limited by ACL and PCL, posterior capsule, anterior horns of menisci. Flexion – Limited by cruciate ligaments and posterior horns of menisci.
Kinematics – Patellofemoral Joint During Flexion 0–90 degrees – Contact area is more central portion of patella. 135 degrees – Medial facet contacts medial femoral condyle. Ideal static – Patella positioned slightly laterally–Remains in trochlear groove until 90 degrees. Extension – Patella moves superiorly along line of femur if VMO and VL are in balance.
Anatomic Impairments Genu Valgum – Femur descends obliquely in a medial direction (normal 5–10 degrees). – Greater load on lateral compartment. – Associated with coxa varum at hip. Genu Varum – Angulation of femur and tibia is 0 or laterally orientated. – Increases load on medial compartment. – Associated with coxa valgum.
Examination and EvaluationComponents of Knee Assessment Pelvis/hip – Muscle length, alignment, performance, capsule mobility Knee – ROM, ligament stability, meniscal tests, extension overpressure response, palpation Patella – Orientation, VMO/VL relationship, lateral retinacular tightness Tibia – Torsion, tibial varum/valgum, rotation Foot – Pronation/supination, rear/forefoot alignment
Muscle PerformanceMuscles commonly tested • Medial and lateral hamstrings • Quadriceps • Gluteal muscles • Iliopsoas • Gastroc-soleus • Hip rotators • Posterior tibialis
Therapeutic Exercise Intervention for Physiologic Impairments Mobility Impairment – Hypomobility • Glide and joint distraction techniques • Patellar mobilization • Quadriceps, hamstring stretches • Abdominal support
Hypermobility • Associated with patellar instability • At risk for ACL injury • Clinical signs – Knee recurvatum and subtalar pronation Treatment • Postural retraining of lower extremity and lumbopelvic region • Co-contraction of lower extremities (high reps-low resistance)
Impaired Muscle Performance Treatment – Strength, endurance, and power training activities. Neurologic Causes: • Lumbar spine injury or disease • MS • Parkinson’s disease
Muscular Strain • Hamstrings and quads most commonly injured. Treatment: • Bleeding control followed by progressive mobility and strengthening. • Plyometrics if within patient’s functional abilities and goals.
Disuse and Deconditioning • Occurs primarily at quadriceps. Treatment: • Strengthening activities for the quadriceps. • Focus on primary cause of disuse.
Therapeutic Exercise for Common Diagnoses – Ligament Injuries ACL • Usually occurs due to hyperextension, deceleration, rotational injury. • Frequently associated with injuries to MCL. Treatment: • Avoid resisted open chain (OC) exercises. • Closed chain (CC) exercises including deceleration, cutting maneuvers, lateral movements, resisted rotational movements, and activities on unstable surfaces.
PCL • Most often a blow to anterior aspect of tibia. • Occasionally, hyperflexion/extension or varus/valgus injury. Treatment: • Avoid open chain exercises. • Closed chain exercises are used.
MCL • Usually torn as a result of valgus stress by a lateral blow or forced abduction of the tibia (skiing). LCL • Much less common than MCL injuries. • Commonly results from hyperextension varus stress. Treatment: • Loading must occur in frontal and transverse planes.
Treatment of Ligament Injuries • Pain can be managed with physical agents, mechanical and electrotherapeutic modalities. • Therapeutic exercise (AROM, PROM). • Joint mobilization may be necessary. • Home program may include exercises to increase ROM and neuromuscular re-education.
Treatment of Ligament Injuries (cont.) • Acute • Aquatics is excellent for: • Mobility, gait, initiating balance, walking, physiologic stretching, leg kicks, toe raises, single leg balance, and squats.
Progression • Continuation training and progressing to non-device-assisted exercises. • Land-based CC exercises.
Late Stage • Resisted OC exercises. • Functional specific drills.
Fractures • Patellar fracture • Distal femur fracture • Tibial plateau fracture • Treatment • Surgically fixated – AROM/PROM exercises for flexion and extension. • Quadriceps and hamstring setting exercises. • Weight-bearing CC exercises – Based on healing and NM control.
Menisci Injuries • Partial meniscectomy • Most often injured traumatically • Degenerative tears Treatment: • Weight-bearing through large ROM should be avoided. • Partial weight-bearing as tolerated is permitted. • Progression is dictated by procedure.
Surgical Procedures • Osteotomy – Treatment is guided by requirements of a healthy joint. Restoring ROM is crucial to ensure proper distribution of loads. • Total knee arthroplasty – Patellar instability can be an issue in 5–30% of TKAs. Limitations at hip and ankle can profoundly affect post-op function.
Tendinopathies Patellar Tendinopathy Treatment • Focuses on patellar tendon’s role in decelerating knee flexion during functional activities. • Stretching exercises are combined with eccentric quadriceps contractions progressing in velocity to match that of daily activities. • OC or CC can be used; however, CC is preferred.
Iliotibial Band Syndrome Treatment: • Postural education • Exercises for underlying impairments (e.g., hip rotator weakness) • Stretching of hip and knee musculature
Patellofemoral Pain Syndrome (PFPS) • Aggravated by knee extension activities. • For example, ascending/descending stairs, squatting, rising from chair, jumping. • Can be caused by frank dislocation, commonly associated with hypermobility of patella, tenderness of patellar borders and femoral condyles, shallow intercondylar groove.
PFPS (cont.) • Overuse. • Poor tracking of patella (shape of osseus surfaces or muscle imbalance). • Q-angle greater in those with PFPS (excessive pronation of foot?) • Greater degree of lateral patellar tilt. • Muscle imbalance (VMO:VL).
PFPS Treatment • General quadriceps strengthening. • All exercises to be performed in pain-free ROM. • Exercises can be CC or OC. • Exercise difficulty is dictated by total target ROM. • Eccentric control exercises are commonly prescribed. • Patellar taping can be helpful.
Summary • Relationships among lumbopelvic, hip, knee, ankle, foot requires thorough evaluation and treatment. • Anatomic impairments can predispose the patellofemoral joint to poor tracking and excessive loads. • Physiologic impairments (mobility, muscle performance, etc.) of neighboring regions can be manifested as symptoms at the knee.
Summary (cont.) • Examination of patellofemoral joint must include muscle length, joint mobility, etc. at neighboring regions and assessment of patellar position and motion. • Improvements in impairments and general quadriceps strengthening within the entire lower kinetic chain associated within PFPS may result in positive outcomes.
Summary (cont.) • Major anatomic impairments at the knee are genu valgum/varum. These postures predispose lateral and medial compartments to excessive loads. • Physiologic impairments at the knee can be compensated by motion at other joints.