Download
1 / 49
660 likes | 1.41k Views
NON HODGKIN’S LYMPHOMA. Sec C Group D Mamba - Medenilla. Non-Hodgkin’s Lymphoma. Heterogenous group of lymphoproliferative malignancies with differing patterns of behavior and responses to treatment Originates in the lymphoid tissues and can spread to other organs Reed-Sternberg cells

E N D
NON HODGKIN’S LYMPHOMA Sec C Group D Mamba - Medenilla
Non-Hodgkin’s Lymphoma • Heterogenous group of lymphoproliferative malignancies with differing patterns of behavior and responses to treatment • Originates in the lymphoid tissues and can spread to other organs • Reed-Sternberg cells • Separated from Hodgkin’s disease • Less predictable • Greater predilection to disseminate to extranodal sites
Non-Hodgkin’s Lymphoma • Can be divided into: • Aggressive (fast-growing) types • Indolent (slow-growing) types • Classification • B-cell • T-cell • Prognosis • Histologic type • Stage • Treatment
Relatively good prognosis • Median survival time:10 yrs • Not usually curable in advanced stages • Early-stage (I and II) indolent NHL • treated effectively with radiation therapy alone • Most of the indolent types are nodular (or follicular) in morphology • It has a shorter natural history • Significant number of patients • cured with combination chemotherapy regimens Indolent Lymphomas Aggressive Lymphomas
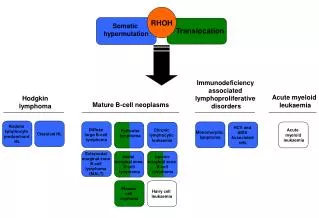
B-cell Non-Hodgkin’s Lymphomas • Precursor B cell Neoplasm • Precursor B-lymphoblastic lymphoma • Mature(Peripheral) B cell neoplasm • B cell Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (CLL/SLL) • B cell prolymphocytic leukemia • Lymphoplasmacytic Lymphoma • Splenic Marginal Zone B cell Lymphoma • Plasma cell myeloma/ Plasmacytoma • Extranodal Marginal Zone B cell Lymphoma of MALT Type • Mantle Cell Lymphoma • Follicular Lymphoma • Nodal Marginal Zone B cell Lymphoma • Diffuse Large B-cell Lymphoma • Burkitt’s Lymphoma
T-cell Non-Hodgkin’s Lymphomas • Hepatosplenic ɣδ T cell Lymphoma • Subcutaneous Panniculitis-like T cell Lymphoma • Mycosis Fungoides/Sezary Syndrome • Anaplastic large cell lymphoma, primary cutaneous type • Peripheral T cell Lymphoma, not otherwise specified • Angioimmunoblastic T cell Lymphoma • Anaplastic Large Cell Lymphoma, primary systemic type • Precursor T cell Neoplasm • Precursor T-lymphoblastic lymphoma • Mature(Peripheral) T cell neoplasm • T cell prolymphocytic leukemia • T cell granular lymphotic leukemia • Aggressive NK cell Leukemia • Adult T cell Lymphoma • Extranodal NK/T cell Lymphoma • Enteropathy-Type T cell Lymphoma
General Aspects of Lymphoid Malignancies Fauci, et al., 2008. Harrison’sPrinciples of Internal Medicine, 17th ed.US:Mcgraw Hill, p. 687
Non-Hodgkin’s Lymphoma Fauci, et al., 2008. Harrison’sPrinciples of Internal Medicine, 17th ed.US:Mcgraw Hill, p. 688
Non-Hodgkin’s Lymphoma • Environmental Factors: • Infectious agents • Chemical exposures • Medical treatments Fauci, et al., 2008. Harrison’sPrinciples of Internal Medicine, 17th ed.US:Mcgraw Hill, p. 688
Non-Hodgkin’s Lymphoma Fauci, et al., 2008. Harrison’sPrinciples of Internal Medicine, 17th ed.US:Mcgraw Hill, p. 688
Non-Hodgkin’s Lymphoma Fauci, et al., 2008. Harrison’sPrinciples of Internal Medicine, 17th ed.US:Mcgraw Hill, p. 688
Immunology • All lymphoid cells are derived from a common hematopoietic progenitor • Sequential activation of a series of TF’s, cells becomes committed to the lymphoid lineage T and B cells
B cells development • A cell becomes committed to the B cell development arrangement of immunoglobulin genes
T cell development • A cell becomes committed to T cell differentiation • upon migration to the thymus • Reaarangement of T cell antigen genes
Malignancies • Associated with recurring genetic abnormalities • At a variety of chromosomal changes • Gross (translocations, additions or deletions) • Rearrangement of specific genes • Underexpression • Mutation of specific oncogenes
Chromosomal translocations • Antigen receptor genes • Immunoglobulin genes on Chr. 2, 14, and 22 on B cells • T cell antigen genes on chr. 7 and 14 in T cells. • Rearrangement to generate mature antigen receptors create a site vulnerability to abnormal recombination
Clinical Features Lymphadenopathy • the most common manifestation of lymphoma • Waldeyer ring & mesenteric Lymph nodes are commonly involved • Spreads in noncontiguous fashion Robbins & Cotran Pathologic Basis of Diseases, 7th edition p. 686
Lymphadenopathy • 2/3 of NHL (and virtually all cases of HL) present with NON TENDER nodal enlargement often >2cm size that can be localized or generalized • The remaining 1/3 of NHL’s arise at extranodal sites ( e.g. skin, stomach and brain) Robbins & Cotran Pathologic Basis of Diseases, 7th edition p. 668
Other Signs And Symptoms • fevers, night sweats, weight loss, and fatigue • pruritus • shortness of breath, chest pain, cough, abdominal pain and distension, or bone pain • pallor (suggesting anemia) • purpura, petechiae, or ecchymoses (suggesting thrombocytopenia) http://emedicine.medscape.com/article/202677-overview Harrison’s Principle of Internal Medicine 17th edition
Robbins & Cotran Pathologic Basis of Diseases, 7th edition p. 671
Robbins & Cotran Pathologic Basis of Diseases, 7th edition p. 671
Robbins & Cotran Pathologic Basis of Diseases, 7th edition p. 671
Lymphoid neoplasia can be suspected from all the clinical features but histological examination of lymph nodes or other involved tissues is required for the diagnosis Robbins & Cotran Pathologic Basis of Diseases, 7th edition p. 668
Staging evaluation for NHL Ann Arbor Staging system is applicable to both Hodgkin’s disease and NHL
Ann Arbor Staging System • PATIENT: 70 y.o. Male • Gradual weight loss • Low grade fever • Anorexia • Body Weakness • Bilateral Cervical Lymph Nodes • Right Axillary Mass • Largest: 3x2cm • Discrete, nontender, movable • Palpable spleen 3cm below L subcostal margin MCL Source: p. 691
Ann Arbor Staging System • PATIENT: 70 y.o. Male • Gradual weight loss • Low grade fever • Anorexia • Body Weakness • Bilateral Cervical Lymph Nodes • Right Axillary Mass • Largest: 3x2cm • Discrete, nontender, movable • Palpable spleen 3cm below L subcostal margin MCL Staging for our patient: Stage III1B Source: p. 691
Ancillary procedures for Primary staging • CBC • ESR • LDH • ß2- microglobulin • Serum protein electrophoresis • Chemistry studies reflecting major organ function • CT scans (chest, abdomen, pelvis) • Bone marrow biopsy Source: p. 692
International Prognostic Index (IPI)for NHL • A powerful predictor of outcome in all subtypes of NHL • Scoring: based on presence or absence of • 5 adverse prognostic factors • may have none or all 5 of these Source: p. 692
ECOG PERFORMANCE STATUS* • PATIENT: 70 y.o. Male • Gradual weight loss • Low grade fever • Anorexia • Body Weakness • Bilateral Cervical Lymph Nodes • Right Axillary Mass • Largest: 3x2cm • Discrete, nontender, movable • Palpable spleen 3cm below L subcostal margin MCL http://ecog.dfci.harvard.edu/general/perf_stat.html
KARNOFSKY PERFORMANCE STATUS SCALE DEFINITIONS RATING (%) CRITERIA • PATIENT: 70 y.o. Male • Gradual weight loss • Low grade fever • Anorexia • Body Weakness • Bilateral Cervical Lymph Nodes • Right Axillary Mass • Largest: 3x2cm • Discrete, nontender, movable • Palpable spleen 3cm below L subcostal margin MCL http://www.hospicepatients.org/karnofsky.html
International Prognostic Index (IPI)for NHL • PATIENT: 70 y.o. Male • Gradual weight loss • Low grade fever • Anorexia • Body Weakness • Bilateral Cervical Lymph Nodes • Right Axillary Mass • Largest: 3x2cm • Discrete, nontender, movable • Palpable spleen 3cm below L subcostal margin MCL Source: p. 692
Precursor B cell Lymphoblastic Leukemia • Remission induction with combination therapy • Consolidation phase: • High dose systemic therapy • Treatment to eliminate CNS disease • Continuing therapy: prevent relapse and effect cure • Combination therapy used: • Rituximab- fludarabine- cyclophosphamide • Associated with grade III or IV neutropenia • Cyclophophamide- vincristine- prednisone • Cyclophosphamide- doxorubicin- vincristine- prednisone
B Cell Chronic Lymphoid Leukemia/ Small Lymphocytic Leukemia • Chlorambucil: orally; few immediate side effects • Chosen in elderly patients who require therapy • Fludarabine: IV; with significant immune suppression • more active agent; with significant incidence of complete remission • Regimens inclusive of this drug is chosen for young patients presenting with leukemia requiring therapy • Second line agent for patients with tumors unresponsive to chlorambucil
B Cell Chronic Lymphoid Leukemia/ Small Lymphocytic Leukemia • Rai stage O and Binet stage A (no manifestations of disease other than BM involvement and lymphocytosis • Followed without a specific therapy • With adequate number of circulating normal blood cells, asymptomatic • Require treatment for the first few years of follow up • Rai stage III or IV or Binet stage C (Bone Marrow failure) • Require initial therapy • Immune manifestations should be managed independently of antileukemic therapy
MALT Lymphoma • Radiation and Surgery • Because it is often localized • Eradication of H. pylori infection • With more extensive diseases: Chlorambucil
Mantle Cell Lymphoma • With disseminated disease: aggressive combination chemotherapy regimens+ autologous/ allogeneic BM transplantation • Localized diseases: combination chemotherapy + radiotherapy • Asymptomatic, elderly patient: observation + single- agent chemotherapy
Follicular Lymphoma • Asymptomatic patient, older patient: watchful waiting • For those who require treatment: single- agent chlorambucil or cyclophosphamide or combination therapy with CVP or CHOP • For patients with localized follicular lymphoma: radiotherapy • Most responsive to chemotherapy and radiotherapy • Active therapies: • Fludarabine • Interferon α: prolong survival in patients on doxorubicin- containing combination therapies • Monoclonal antibodies with or without radionuclides • Lymphoma vaccines
Diffuse Large B Cell Lymphoma • Initial Treatmant: combination chemotherapy regimen= CHOP + Rituximab • Stage I or non bulky stage II: 3-4 cycles + field radiotherapy • Bulky stage II, stage III, stage IV: 6-8 cycles or 4 cycles then reevaluate -> complete remission -> 2 more cycles, then therapy discontinued • IPI : predict favorable responses • Score 0-1: 5 year survival >70 % • Score 4-5: 5 year survival ~20% • For refractory cases or relapse • Salvage therapy • Alternative combination therapy • Autologous bone marrow transplantation
Burkitt’s Lymphoma • Treatment should begin 48 hrs after diagnosis • High doses of Cyclophosphamide • Prophylactic therapy to CNS mandatory
Other B Cell Lymphoid Malignancies • Hairy cell leukemia: Cladribine • Splenic marginal zone lymphoma: splenectomy, chlorambucil • Lymphoplasmacytic lymphoma: Chlorambucil, fludarabine and cladribine • Nodal marginal zone lymphoma: treatment same as follicular lymphoma
Precursor T Cell Lymphoblastic Leukemia • Very intensive remission induction and consolidation regimens • Leukemia- like regimens: for older children and young adults • With high levels of LDH or BM, CNS involvement: BM transplantation
Anaplastic Large T/ Null Cell Lymphoma • Treatment regimens same as for other aggressive lymphomas (diffuse large B cell lymphoma) • Rituximab is omitted
Mature/Peripheral T Cell Disorders • MycoisesFungoides • Localized early stage: radiotherapy- total skin electron beam irradiation • More advanced disease: topical glucocorticoids, topical nitrogen mustard, phototherapy, psoralen with PUVA, electron beam radiation, IFN, Antibodies, fusion toxins and systemic cytotoxic therapy • Adult T Cell Lymphoma/ Leukemia • Combination chemotherapy regimens