Download
1 / 27
270 likes | 628 Views
Perinatal Varicella. By Rafat Mosalli MD FAAP FRCPC. Objectives. Perinatal varicella related diseases How common is it How to prevent Congenital and neonatal form Indication of VZIG Hospital isolation and precaution methods for infected mother and exposed newborn. Problem 1.

E N D
Perinatal Varicella By Rafat Mosalli MD FAAP FRCPC
Objectives • Perinatal varicella related diseases • How common is it • How to prevent Congenital and neonatal form • Indication of VZIG • Hospital isolation and precaution methods for infected mother and exposed newborn.
Problem 1 • You are called to assess a newborn that his mother has a history of Chicken pox 3d prior to delivery, you will: • Isolate the baby and start VZIG as soon as possible together with acyclovir • Isolate the baby and start treatment with acyclovir • Isolated the baby and give VZIG only • No treatment is indicated since the risk is low.
Problem 2 The type of isolation needed for the newborn whose mother developed chickenpox 5 days prior and 2 days post to delivery is: 1- Standard, contact and airborne precaution. 2-only standard and airborne 3- Only Contact. 4-No isolation is needed.
Problem 3; In regard to VZIG all true except: 1- VZIG does not prevent 100% of cases of neonatal varicella 2- Best given within 96 hours of exposure 3- Not effective once active disease occurs 4- it is indicated for newborn with onset of maternal varicella within 5 days prior through 2 days following delivery 5-VZIG may shorten the incubation period.
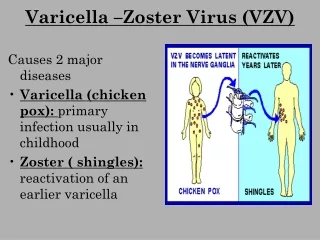
Varicella Zoster Virus (VZV) -Causes chicken pox and shingles - Humans are the only known reservoir - Highly contagious - Transmission is by contact or airborne droplets
Epidemiology • Exposure to a household results in infection in virtually all susceptible members • Incubation period usually 14-16 days Can range 10-21 days • Patients are contagious from 2 days prior to and 5 days after the onset of the rash • Immunocompromised patients contagious for duration of rash
Perinatal varicella related disease • Maternal Varicella • Congenital varicella • Neonatal varicella
Varicella and pregnancy • Varicella in pregnancy is relatively rare (5 per 10,000) • Severe form (maternal pneumonia ,congenital infection, abortion) • IgG, IgM, and IgA are produced within 2 to 5 days after infection ,The IgG crosses the placenta to provide passive immunity to the fetus . • All exposed pregnant women not having a history of varicella should be tested for antibody, although most are immune
Post-exposure pregnancy prophylaxis • (VZIG) is recommended within 96 hours of exposure of a pregnant woman who is non-immune to VZV. • VZIG is also recommended if it is not possible to obtain antibody test results within 96h.
Post-exposure pregnancy prophylaxis • The dose recommended by the manufacturer is 125 U (1 vial) per 10 kg, with a maximum of 625 U . • No prospective studies evaluating the efficacy of VZIG or acyclovir for the prevention of congenital varicella. • 90% effective in preventing severe varicella infection in exposed pregnant women
Varicella and pregnancy Treatment for mother : • Isolation, supportive • Monitor for pneumonia • oral acyclovir (Class C drug by FDA) :administered at 24 hours after rash onset • Early acyclovir has been used to limit the course of illness during pregnancy
2-Congenital Varicella • Caused by maternal infection in the 1st • trimester to early 2nd trimester • Greatest risk between 13-20 weeks gestation • Overall attack rate 1.2% • Limb atrophy and scarring • Chronic encephalopathy and cortical Atrophy, Chorioretinitis, micropthalmia, cataract
Prenatal diagnosis • Is difficult and invasive. • Benefit/risk is low • Noninvasive with ultrasound: cranial calcifications, porencephalic cysts, hepatic calcifications ,echogenic bowel, ascites, hydrops, and polyhydramnios…
3-Neonatal Varicella • Transplacental exposure • At risk when mother develops varicella from 5 days prior to 2 days after delivery • Can manifest from 1-16 days after delivery • High risk for disseminated varicella • Mortality rates as high as 30% • Prognosis much better if lesions develop greater than 5 days after delivery
3-Neonatal varicella • of varying severity (mild systemic). • Treatment with VZIG . • VZIG does not prevent 100% of cases of neonatal varicella • In one series : half of the infants who received prophylaxis developed chickenpox, though the severity of the infection was reduced
Nosocomial Transmission • Well documented in pediatric wards • Rare in newborn nurseries High risk infants: • Premature infants (> 28 weeks gestation and > 1000 grams) whose mother has no history of varicella • Premature infants (< 28 weeks gestation or < 1000 grams) regardless of maternal history
Nursery control measures -Siblings 14 years of age or less, check their immunization status. Siblings who have not had chickenpox or the vaccine are not allowed to visit, -Adult visitors who have been in contact with chicken pox(3 w) and/or unsure of their immune status must not visit until they are shown to be immune
Varicella Zoster ImmuneGlobulin (VZIG) • Provides passive immunity • Not effective once active disease occurs • Dosage: 125 units/10 kg • Minimum dose: 125 units • Maximum dose: 625 units • Never administer intravenously • Best given within 96 hours of exposure
Indications for VZIG (assumingsignificant exposure) • Susceptible pregnant women • Newborn with onset of maternal varicella within 5 days prior through 2 days following delivery • Hospitalized premature > 28 weeks gestation and no maternal history of varicella • Hospitalized premature < 28 weeks gestation or <1000 grams regardless of maternal history
VZIG • Term infants exposed after 2 days of life are • not at increased risk • VZIG not indicated • All infants who receive VZIG should be in strict isolation • 50% of infants still develop varicella though disease tends to be milder • VZIG may prolong incubation as long as 28 d
Isolation of the hospitalized patient • For Infected Mother: standard+ airborne+ contact precaution for a minimum 5d after the onset of the rash till all lesions crusted. • For neonates of infected mother: standard +airborne+ contact precaution till 21d if still hospitized(28 d if had IG) • For infant with congenital varicella: No need for isolation
Summary • Fortunately, varicella in pregnancy is relatively rare with only 1.2% Fetal attack rate ,nevertheless; complications (Maternal & fetal) can be severe. • Treatment of neonatal form with VZIG . • Remember the indications of VZIG.
The message for Obstetrician and internist Prevention is Important: • Physicians caring for women have the opportunity to prevent the complications of varicella by identifying and vaccinating susceptible women. • With the introduction of the varicella vaccine and its efficacy, the rate of varicella in pregnancy isexpected to decrease dramatically.