Download
1 / 64
640 likes | 718 Views
Bone infection, or osteomyelitis, is an inflammation caused by infective organisms leading to bone destruction. Learn about the classification, risk factors, causes, pathogenesis, symptoms, diagnosis, treatment, and complications of this condition.

E N D
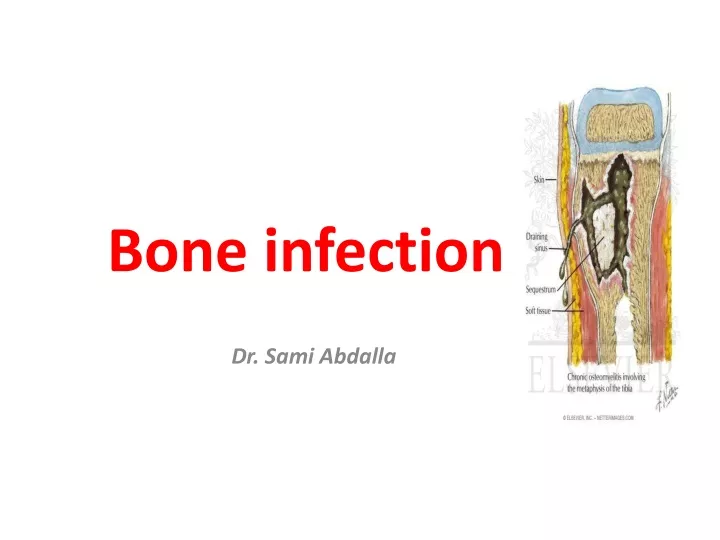
Bone infection Dr. Sami Abdalla
Definition • An inflammation of the bone caused by an infective organism, leading to inflammatory destruction of bone, necrosis and new bone formation.
Classification • Based on : • Duration and type of symptoms. • According to the mechanism. • Host response.
Risk factors • Systemic: • Malnutrition. • Sickle cell anaemia. • Diabetes. • Immuno-suppressive conditions. • Local: • Trauma. • Foreign body. • contiguous infection.
Causal organism: • Staph. aureus 80% • Strept., Pneumococcus, H. infleunzae (<2yrs), • Pseudomonas heroin addicts. • Salmonella sickle cell anaemia.
Sources fo infection • Minor skin abrasion, boil, septic tooth. • Infected umbilical cord. • Urethral catheterization.
Pathogenesis • The organism usually settle in the metaphysis of : • Proximal tibia. • Proximal and distal femur. • Proximal end of the humerus.
Acute inflammatory reaction: • Increase intra-osseous pressure. • Obstruction to the blood flow. • Intravascular thrombosis.
Suppuration: • Pus forms within the bone in the 2nd and 3rd day. • Through volkman’s canal subperiosteal abscess forms.
Bone necrosis: • By the end of the first week. • Due to • infective thrombosis • Periosteal stripping. • Bacterial toxin. • Leucocyte enzymes.
New bone formation; • By the end of the 2nd week.
Clinical features • Constitutional symptoms. • Severe pain. • Tenderness, • Lymphadenopathy. • In adult backache and mild fever.
Investigation • Blood culture +ive in 50% . • Blood test. • Culure aspirate. • Ulrasoud. • M.R.I. • Radiography. • Bone scan.
Differential diagnosis • Cellulitis. • Strep. Necrotizing myositis. • Acute suppurative arthritis , • Acute rheumatism. • Sickle cell crisisl • Gaucher’s disease.
Treatment • Supportive treatment. • Splintage • Antibiotic therapy • Best guess. • Gm stain. • Culture and sensitivity.
Surgical treatment; • Unresponsiveness within 36 hrs of starting treatment. • Signs of deep pus.
Complication • Septicaemia.( rare). • Metastatic infection ( infants) • Suppurative arthrits. • Altered bone growth. • Chronic osteomyelitis.
Differ from AHO in severity of symptoms and signs. • Common in distal femur, proximal and distal tibia. • Staph. Aureus and epidermis are the predomint organisms.
Clinical picture • The patient is usually a child or adolescent. • Pain for severa weeks or even months. • Mild constitutional symptoms. • Limping and slight swelling. • Muscle wasting and local tenderness.
This indolent course is due to • increase host resistance. • Lower bacterial virulence. • Antibiotic administration.
Investigation • TWB normal. • ESR 50% • Blood culture usually are not +ive. • Culture of bone aspirate or biopsy 60%. • X-ray.
Treatment • Conservative : • For typical lesions. • Antibiotics for 6/52.
Biopsy and curretage; • For aggressive lesion. • If the diagnosis is in doubt.
Most common cause in adults. • Common organisms • Staph.aureus. • Gm –ive coliform. • An aerobic organisms,
Clinical picture • Constitutional symptoms. • Sero-purulent discharge. • Delayed union. • Leucocytosis and increase in ESR
Treatment • Prophylaxis. • Cleaning and debridement of open # • Provision of drainage by leaving the wound open. • Immobilization of the # • Antibiotics.
Pyogenic wound infection; • Regular wound dressing. • Debridement. • External fixation for unstable fracture. • If these failed: • The management is essentially that of chronic osteomyelitis.
Chronic osteomyelitis • Used to be due to acute haematogenous osteomyelitis, but nowadays it more frequently follows an open fracture or operation. • The usual organisms (mixed infection) are staph.aureus, E.coli, strept.pyogenes, proteus and pseudomonos.
Chronic osteomyelitis • Pathology: • The disease may take one 2 forms: • Pus + sequestrum surrounded by vascular tissue beyond which is an area of sclerosis. Sequestra act as substrates for bacterial adhesions, ensuring persistence till they are removed or discharged through a draining sinus
Chronic osteomyelitis • Two factors are responsible for the chronicity of the disease : • presence of dead infected bone • the intra-osseous cavity can’t be obliterated because of the rigid walls and as a result, the body’s normal defense mechanisms and antibiotics are unable to reach all the bacteria in the bone
Chronic osteomyelitis • Brodie’s abscess: • This form is closely contained creating chronic abscess within the bone (pus or jelly-like granulation tissue) surrounded by sclerotic bone. This may be a sequel to pyogenic septicemia from which the pt has recovered but stayed dormant for years or may be found in a pt which is known to have had osteomyelitis affecting a bone other than in which Brodie’s abscess is discovered
Chronic osteomyelitis • Clinical Features: It may remain quiescent for months or years with acute and subacute attacks (flares) i.e. • recurring pain • local • Transitory effusion • Pyrexia and tenderness • Discharging sinus (seropurulent) • In long standing cases, tissues may be puckered in where a scar or sinus is attached
Chronic osteomyelitis • Investigations: • ↑ESR & TWBCs during acute flares • ↑ASO titre • C&S
Chronic osteomyelitis • Radiography is diagnostic: • The classical picture of bone resorption (as patchy loss of density or frank excavation) with thickening and sclerosis of the surrounding bone. However there is marked variations (no more than localized trabeculation, or an area of osteoporosis, or periosteal thickening)
Chronic osteomyelitis • Bone scan: increased activity • CT and MRI: • extent of bone destruction • Reactive edema • Hidden abscesses and sequestra
Chronic osteomyelitis • Treatment: • Antibiotics • Exacerbations are treated by immobilization and antibiotics but only to recur again • It is also used to stop spread of infection to healthy bone • Local treatment: • Sinus: dressing • Abscess: drainage
Chronic osteomyelitis • Operation: • Waiting policy. • The objective is removal of dead bone and elimination of dead space • Under antibiotic cover, all infected soft tissue and all dead bone must be excised • Dead material can be identified by pre-op injection of sulphan blue or probing a sinus or by radiograph • Access to the bone is usually through a previous scar
Chronic osteomyelitis • Double-lumen tubes are laid in the resulting cavity and the tissues are closed with the tubes emerging through separate stab wounds. an appropriate antibiotic solution is instilled 4-hourrly and cleared shortly before the next procedure by low pressure suction. Cavity injection and drainage should be cont. until the effluent is sterile (usually 3-4 weeks). The tubes are then gradually withdrawn as the cavity diminishes in size. • Gentamicin –impregnated beads
Chronic osteomyelitis • Driange tube • (double lumen tube)
Chronic osteomyelitis • Dead space is obliterated by packing the cavity with cancellous bone chips or local muscle flap. • Amyloid disease is taken into consideration when copious amount of pus has persisted for years • Amputation: if exacerbations are frequent and prolonged. • Brodie’s abscess should be treated by evacuation and curettage of the cavity under antibiotic cover. If the cavity is of moderate size, packing with cancellous bone chips is used.
Chronic osteomyelitis • Aftercare: Success is difficult. • prognosis should always be guarded • The watchword is cautious optimism and after all, probable cure is better than no cure.