Download
1 / 24
620 likes | 2.12k Views
PEPTIC ULCER disease (PUD). Dr. Gehan Mohamed Dr. Abdelaty Shawky. Learning Objectives. Recognize the typical clinical presentation and risk factors for peptic ulcer disease. Understand pathophysiology of PUD focusing on H. pylori.

E N D
PEPTIC ULCER disease (PUD) Dr. Gehan Mohamed Dr. Abdelaty Shawky
Learning Objectives • Recognize the typical clinical presentation and risk factors for peptic ulcer disease. • Understand pathophysiology of PUD focusing on H. pylori. • List the four layers of peptic ulcer seen by microscope. • Identify the complications of PUD.
Ulcers are defined as a breach in the mucosa of the alimentary tract, which extends through the muscularis mucosa into the submucosa or deeper. ( An erosion differs from an ulcer in being more superficial than ulcers and partially affecting surface epithelium).
Definition of peptic ulcer: • Peptic ulcers are chronic most often solitary, lesions that occur in any portion of the gastrointestinal tract exposed to the aggressive action of acid-peptic juices.
* Clinical presentation: • Relapsing lesion • Most often diagnosed in middle aged to older adults but may first become evident in young adult life. • Epigastric burning or aching pain. • Pain worse at night and 1 to 3 hours after meal specially in doudonal ulcer.
May radiate to the back (consider penetration) • Relieved by antacids (duodenal), or vomiting (gastric). • Dyspepsia. • Nausea, vomiting, bloating , and weight loss occur. • Hematemesis or melena with GIT bleeding.
* Sites of peptic ulcer: • Duodenum: First portion. Anterior wall is more often affected. • Stomach: Usually antrum. Lesser curvature (common) . • At the margins of a gastroenterostomy (stomal ulcer) • In the duodenum, stomach or jejunum of patients with Zollinger-Ellison syndrome. • Within Meckel’s diverticulum that contains ectopic gastric mucosa.
* Pathogenesis of peptic ulcer: Peptic ulcers are produced by an imbalance between the gastro-duodenal mucosal defense mechanisms and damaging forces.
* Mucosal defense mechanisms: • Bicarbonate secretion • Mucous secretion • Tight adherence between epithelial cells to prevent any acid leakage to the inside. • Good blood supply to the mucosa • Renewal of damaged epithelial cells.
* Damaging agents: • H. pylori • Gastric acid • Pepsin • Superimposed injury from environmental or immunologic agents.
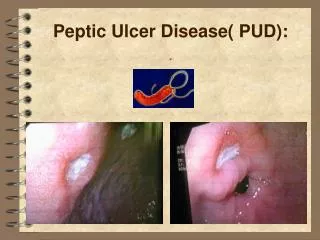
Role ofH. Pylori infection in the pathogenesis of peptic ulcer: H. pylori infection is present in almost all patients with duodenal ulcers and 70% of cases with gastric ulcers. * Mechanism: 1. H. pylori secretes urease (generates ammonia), protease (breaks down glycoprotein in the gastric mucus) or phospholipases. 2. Bacterial lipopolysaccharide attracts inflammatory cells to the mucosa. Neutrophils release myeloperoxide. 3. A bacterial platelet-activating factor promotes thrombotic occlusion of surface capillaries.
Damage of the protective mucosal layer. The epithelial cells are exposed to the damaging effect of acid-peptic digestion. • Inflammation of the gastric mucosa. • Chronically inflamed mucosa more susceptible to acid- peptic injury and prone to peptic ulceration.
* Other Causes of peptic ulcer: • Chronic use of NSAIDs (aspirin) an corticosteroids. • Cigarette smoking. • Psychological stress. • Ischemia.
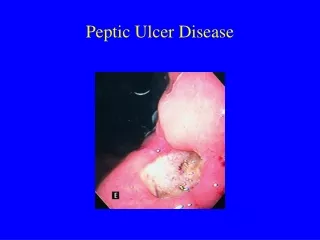
* Gross features: Site: Gastric ulcers are located at the antrum toward the lesser curvature. The duodenal ulcer is usually located at the 1st part anteriorly. Shape: Round, oval. Size: Usually less than 2cm in diameter. • Lesions less than 0.3 cm are likely to be shallow erosions. • Giant ulcers are usually greater than 3cm in diameter. • Size does not differentiate benign from malignant ulcer.
Base of ulcer: • Firm (formed of bundles of muscles and fibrous tissue). Floor: Clean (gastric juice digest any food particles at the floor. Margin (Surrounding gastric mucosa): Edematous and reddened due to gastritis. Depth of the ulcer: • Superficial ulcer penetrate the mucosa reaching up to the muscularis mucosa. • Deeply excavated ulcers having their bases on the muscularispropria.
Biopsy of peptic ulcer • Biopsy is necessary to distinguish between benign and malignant ulcers. • Biopsy should be taken from the ulcer edge, at least from each quadrant. • Up to 10-12 biopsies may be taken to exclude cancer.
* Microscopic features: - Four distinct layers are present in a peptic ulcer in the same sequence starting from the luminal side : 1. Surface coat of exudate and necrotic debris. 2. Fibrinoid necrosis. 3. Granulation tissue. 4. Fibrosis replacing the muscle wall and extending into subserosa.
* Complications of PUD : 1. Hemorrhage: hematemesis or melena. 2. Perforation 3. Healing by fibrosis causing obstruction. 4. Malignant transformation: rare (0.5% of gastric peptic ulcer).