Download
1 / 17
170 likes | 364 Views
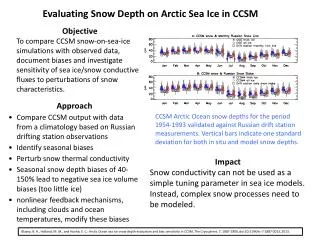
Objective. To assess the impact of the increasing use of MDCT angiography in the setting of blunt and penetrating neck trauma on the use of digital subtraction angiography (DSA). Background of the Study.

E N D
Objective • To assess the impact of the increasing use of MDCT angiography in the setting of blunt and penetrating neck trauma on the use of digital subtraction angiography (DSA)
Background of the Study • Although digital subtraction angiography (DSA) is still accepted as the gold standard for imaging the major vessels of the neck, the reported high number of patients with negative results and the risk associated with performing such procedures have prompted a search for other less invasive imaging techniques. • Noninvasive techniques that have been explored as a potential replacement for catheter angiography in this patient population include MR angiography, duplex sonography, and CT angiography.
Background of the Study • In recent years, CT angiography has also been reported to be useful in the detection of injuries to the major arteries. • Prior studies using single-detector helical CT have shown high sensitivity and specificity for detecting injuries to major vessels of the neck in the setting of both blunt and penetrating trauma.
Patient Population • In general, the patient is considered to be at risk for having an arterial injury and a candidate for diagnostic angiography if one or more of the following signs or symptoms are present: • active bleeding from an unknown source • stable or expanding neck hematoma • neck pain with focal neurologic deficit • palpable bruit or thrill
Methodology • Retrospective: 36 months (Jan 2001 – Dec 2003) • January 2001 to December 2003, 57 patients were referred for CT angiography or DSA of the neck after blunt or penetrating neck trauma • All CT angiograms were acquired with a 4-MDCT scanner • The patients were divided into three groups on the basis of consecutive 12-month periods (2001, 2002, and 2003), and the initial imaging technique was recorded • The results of CT and digital subtraction angiograms were compared with operative findings and with clinical course, when available.
Methodology • Of the 57 patients, 17 underwent both MDCT angiography and DSA during the study period. • The mean age of the study population was 31 years with an age range of 14–90 years. • The mechanism of injury in the study population included gunshot wound (n=21), stab wound (n=12), motor vehicle crash (n=12), assault with a blunt object (n=4), attempted hanging (n=2), fall (n=3), crush injury (n=1), and twisting injury (n=2).
Methodology • CT angiography examinations were reported as positive when one or more of the following findings were present: • arterial dissection, arterial pseudoaneurysm, arterial transection, or arterial occlusion. • Findings were reported as indeterminate if isolated IV contrast extravasation was present without an identifiable arterial injury on the CT images
Results • In 2001, 12 patients were referred for imaging: nine patients were evaluated initially with DSA and three patients were evaluated with CT angiography and subsequently with DSA for further evaluation. • In two of these three patients, CT angiograms showed no abnormality and this result was confirmed with catheter angiography • The third patient underwent DSA for suspected pseudoaneurysm of the superior thyroidal branch of the external carotid artery based on findings present on the initial CT angiography; DSA confirmed this finding
Results • In 2002 and 2003, 11 and 34 patients, respectively, underwent CT angiography as the initial imaging examination. During these 2 years, no patient underwent DSA as the initial diagnostic test, but five patients underwent DSA after CT angiography for the following indications: • evaluation of nondiagnostic CT angiograms (n=1) • confirmation of findings when requested by the clinical service (n=2) • and catheter-guided therapy (n=2)
Results • 2002 • Of the 11 CT angiography examinations, one patient with a gunshot wound to the neck was found to have an occlusion of the left internal carotid artery and dissection of the left vertebral artery • Another patient with a large laceration from a stab wound had negative findings on the initial CT angiogram. This patient was taken to the operating room for wound exploration before repair of the laceration, and a facial vein laceration was repaired • Nine other patients with negative CT angiography findings were managed conservatively, without further intervention or diagnostic imaging
Results • 2003 • Of the 33 diagnostic CT angiograms, five were reported as positive for arterial injury. • pseudoaneurysm and dissection (n=1), pseudoaneurysm and occlusion (n=1), iso- lated pseudoaneurysm (n=1), isolated occlu- sion (n=1), and pseudoaneurysm with occlu- sion and active extravasation (n=1) • Isolated contrast extravasation was reported as indeterminate for arterial injury in three patients • In one patient, a right common carotid artery pseudoaneurysm was identified on initial CT angiography, and catheter angiography was requested. On confirmation of the findings, the patient underwent operative repair.
Results • 2003 • In the remaining 25 patients in whom the initial CT angiography findings were considered negative, two patients were explored surgically despite negative CT angiography findings because of a high clinical suspicion for vascular injury based on the mechanism of injury • in both cases, no vascular injury was identified • Three other patients were subsequently imaged using MR angiography of the head and neck for evaluation of suspected intracerebral vascular pathology as a cause for persistent neurologic systems • all MR angiograms were interpreted as negative.
Summary of Results • During the 3-year period of this retrospective study, eight (14%) of 57 patients in the study population had vascular injuries. When CT angiography was performed as the initial im- aging examination, seven (15%) of 48 patients had cervical arterial injuries.
Discussion • DSA is the generally accepted gold standard for evaluating the major vessels of the neck and, until recently, has also served as the initial imaging examination requested by trauma and vascular surgeons when such injuries are suspected • However, the small but appreciable risks associated with DSA, the extended procedure time, and the additional staff required to perform this procedure have led to a search for other potential imaging diagnostic techniques
Discussion • Unlike MR angiography, CT angiography is generally available in most emergency radiology departments and can be performed at the time of diagnostic imaging for other organ systems in the patient with multiple injuries from trauma. • Even when MR angiography is available immediately, the time needed for the examination may be prohibitive even in hemodynamically stable patients. • In addition, flow effects, artifacts, and limited spatial resolution compared with CT may limit the sensitivity of MR angiography for detecting clinically significant injuries. • CT angiography offers advantages over color Doppler sonoraphy including lack of operator dependence and ability to image patients with difficult anatomy or with neck hematomas that are not easily amenable to sonographic scanning
Conclusion • The advent of MDCT allows improved spatial resolution, and the diagnostic potential of CT angiography in the acute trauma patient will undoubtedly increase with the introduction of CT scanners with more than 16 detector rows • CT angiography has essentially replaced DSA as the study of choice for the initial evaluation of the neck vessels in the setting of blunt or penetrating trauma. • Only a minority of patients will require DSA after CT angiography for therapeutic interventions or for further diagnostic investigation when initial results are equivocal or nondiagnostic. • CT angiography allows appropriate triage of patients to conventional angiography or surgery for appropriate treatment and can guide conservative management when appropriate.