Download
1 / 45
450 likes | 459 Views
Explore the risk factors and genetic causes of colon cancer, learn about screening and preventive strategies, and understand the role of chemoprevention and targeted therapies in colon carcinogenesis. Discover the stages, treatments, and trends in colorectal cancer management.

E N D
Lalan S. Wilfong GI malignancies May 28, 2009
Colon Cancer • 800,000 new cases per year globaly • 11% of cancer mortality in the US • Lifetime risk of 0.5-2.0% of developing colon cancer • Risk factors • Age, Western countries, high-fat diets • Obesity, Genetics, Inflammatory Bowel Disease
Genetic Causes • Familial Adenomatous Polyposis • Hereditary Nonpolyposis Colorectal Cancer • Hamartomatous Polyposis Syndromes • Familial Colorectal Cancer
Familial Adenomatous Polyposis • 1% of all colorectal cancer • Hallmark is hundreds to thousands of colon polyps • 100% develop colon cancer • Extracolonic features: • Hypertrophy of retinal epithelium • Mandibular osteomas • Epidermal cysts • Desmoid tumors • Adrenal cortical adenomas • Gene is APC on 5q21
3% of colorectal cancer Usually occurs in right colon Accelerated progression of polyps to cancer Can have extracolonic tumors Risk: 80% for colon cancer 40% for endometrial With skin tumors called Muir-Torre syndrome Autosomal dominant with 80% penetrance Defect in mismatch repair genes Can test for Microsatellite instability in tumors HNPCC
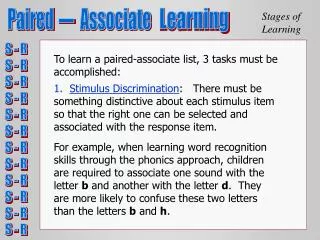
What Happens? • Mismatch Repair genetic defect • Encode enzymes that repair errors during DNA replication • Main genes MLH1, MSH2, MSH6 and PMS2 • Microsatellite instability • Microsatellites are repetitive DNA sequences found throughout the genome • Loss of MMR results in repetitive coding and noncoding regions of genes including genes involved in tumor initiation and progression
Putative Role of Mutations in Mismatch-Repair Genes Lynch, H. T. et al. N Engl J Med 2003;348:919-932
Strategy for Risk Reduction • Colonoscopy every 1-3 years beginning age 20-25 or 10 years before earliest relative • Prophylactic colectomy • Chemoprevention? • Transvaginal ultrasound or endometrial aspiration annually • Prophylactic hysterectomy • If stomach cancer in family, EGD every 1-2 years • If urinary tract cancer, sono or urine cytology every 1-2 years
Slow progression from adenoma to cancer make screening appropriate Best approach is unknown DRE Fecal occult blood Sigmoidoscopy Barium enema Colonoscopy Average Risk FOBT Flex sig every 5 yrs Colon every 10 yrs Stop at age 75-85 Increased Risk Colon starting 10 years before youngest affected member 3 or more polyps, colon in 3 years 1-2 polyps (<1cm) colon in 5 yrs Screening for Population
Chemoprevention • Medications to prevent cancer before cancer begins • Since colon cancer has stepwise progression from adenoma to invasive disease, if we can block one of the steps we can stop cancer
Colon Carcinogenesis and the Effects of Chemopreventive Agents Janne, P. A. et al. N Engl J Med 2000;342:1960-1968
I II III IV Stage • T • 1: invades submucosa • 2: invades muscularis propria • 3: through muscularis propria • 4: invades other organs • N • 0: no lymph nodes • 1: 1-3 lymph nodes • 2: 4 or more lymph nodes • M: • 0: no mets • 1: with mets
Treatment • Stage I – surgery • Stage II – surgery unclear role of chemotherapy • Stage III – surgery followed by adjuvant chemotherapy • Stage IV – palliative chemotherapy • Rectal Cancer – surgery, radiation and chemotherapy
Disease-free survival after adjuvant chemotherapy for colorectal cancer using Fluorouracil and Leucovorin (FL) or FL + Oxaliplatin Andre, T. et al. NEJM 2004; 350:2343-2351
Trends in the Median Survival of Patients with Advanced Colorectal Cancer Meyerhardt, J. A. et al. NEJM 2005; 352:476-487 Adapted from Grothey et al
Targeted Therapies • Avastin • VEGF inhibitor • Blocks blood vessel formation • All cells need O2 and therefore blood • Erbitux/Vectibix • EGFR inhibitor • Overexpression in many cancer cell lines • Important ligand for growth factors
Angiogenesis • Cells cannot survive ifthey lack oxygenand nutrients • Oxygencan diffuse from capillaries to a distance of only 150 to 200µm • when cells are farther away from a blood supplytheydie. • Thus, to become clinically relevant, a tumor requires neovascularization or angiogenesis to survive
Epidermal Growth Factor Receptor Inhibitor • EGFR overexpressed on many epithelial cancers • Correlates with poor outcome • Acts as a tyrosine kinase • Blocking this receptor can lead to cell cycle arrest and apoptosis • EGFR blockade can improve survival in many cancers • Only effective in tumors with wild-type kras
Fig 1. Mechanisms of receptor activation Mendelsohn, J. J Clin Oncol; 20:1s-13s 2002
Esophageal Cancer • 12,000 cases in US per year • More common in Asia, blacks, males, age >50 • Two Cell Types • Squamous – • associated with smoking, etoh, nitrities, pickled vegetaqble, lye, achalasia, esophageal web, diet • Incidence decreasing • Adenocarcinoma – • associated with reflux, Barrett’s, obesity • Incidence increasing esp in white males
Location 15% upper 1/3 40% middle 1/3 45% lower third Symptoms Dysphagia Weight loss Pain vomiting Spread Adjacent lymph nodes Lung Liver Pleura Diagnosis Endoscopy CT scans PET Clinical Features
Treatment • Most patients present with advanced disease and prognosis is <5% 5 year survival • Resection for early stage disease • Chemoradiation for locally advanced disease • Chemotherapy for advanced disease • PEG tube or stents for nutrition
Gastric Cancer • Incidence decreasing • 21,500 new cases per year • More common in Asia • 85% adenocarcinomas • Diffuse – infiltrate and thicken the stomach wall causing linitis plastica • Intestinal type – glandlike structures
Etiology Ingestion of nitrates H pylori Loss of gastric acidity Presentation Upper abdominal pain Anorexia +/- nausea Weight loss dysphagia Spread Directly to perigasatric tissues Peritoneal seeding Intra-abdominal and supraclavicular lymph nodes Ovary (Krukenberg) Periumbilical (sister Mary Joseph) Peritoneal cul-de-sac (Blummers shelf) Liver Features
Treatment • Resection for early stage • Lymph node dissection • 20% 5 year survival • Palliative even in advanced disease • Chemotherapy for advanced disease • Palliative benefit • ? Prolongs survival • Radiation only for palliation
Pancreatic Cancer • Incidence increasing – 28,299 cases in 2000 • Risk factors • Smoking • Age • Male • Blacks • Chronic pancreatitis • Diabetes • obesity
Treatment • Resection • Only 15% have resectable lesions • 5 year survival 10% • Maybe improved with chemoradiation • Unresectable or metastatic • Survival 6 months • Chemo offers palliation
Clincal Features • 90% adenocarcinomas • 70% in head, 30% in body and tail • Onset insidious • Jaundice • Pain • Weight loss • Diagnosis • Ct scan • MRI • EGD, ERCP, EUS • Ca 19-9
Median Survival: 18.8 months with Gemzaar vs. 16.7 months for 5-FU
Current Research at PHD • Colon Cancer • SPIRITT: Folfiri with panitumimab or avastin 2nd line MCRC in kras wild-type • Folfiri +/- AMG479 or AMG 655 or placebo in 2nd line kras mutant colon cancer • Gastric • Docetaxel and Oxaliplatin +/- cetuximab for metastatic gastric adenoca • Pancreatic • Gemcitabine +/- amplimexon for met pancreatic cancer • Gemcitabine +/- GI-4000 for resected pancreatic cancer



![CP = E[ s 2 , s 5 , s 1 , s 3 , s 2 ’ , s 3 ’ , s 4 , s 1 ’ , s 4 ’ , s 5 ’ ] S[] I[]](https://cdn3.slideserve.com/6546826/slide1-dt.jpg)