Download
1 / 10
100 likes | 149 Views
Splinting and Use of Crutches. Emergency Emotional Care. Emergency care relative to emotional reactions to trauma must be provided Accept rights to personal feelings Show empathy, not pity Accept injured person’s limitations as real Accept own limitations as provider of first aid Be calm.

E N D
Emergency Emotional Care • Emergency care relative to emotional reactions to trauma must be provided • Accept rights to personal feelings • Show empathy, not pity • Accept injured person’s limitations as real • Accept own limitations as provider of first aid • Be calm
Emergency Splinting • Should always splint a suspected fracture before moving • Use proper immobilization to decrease risk of • Damage • Hemorrhage • Potential for death (if handled improperly) • Splint where athlete lies and avoid moving them • Splint one joint above and one below fracture
Rapid form immobilizer • Styrofoam chips sealed in airtight sleeve • Moldable with Velcro straps to secure • Air can be removed to make splint rigid • Air splint • Clear plastic splint inflated with air around affected part • Can be used for splinting but requires practice • Do not use if it will alter fracture deformity • Provides moderate pressure and can be x-rayed through • Half-ring splint • Used for femoral fractures • Requires extensive practice • Open fractures must be dressed appropriately to avoid contamination
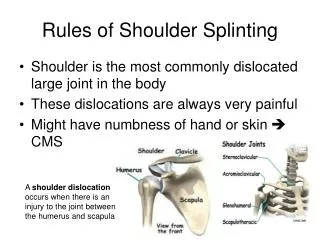
Lower Limb Splinting • Foot and ankle require splinting of foot and knee • Knee, thigh, or hip require splinting of whole leg and one side of trunk • Upper Limb Splinting • Shoulder splinting is difficult • Use sling and swathe with upper limb bound to body • Upper arm and elbow • Splint with arm straight to lessen bone override • Lower arm and wrist • splint in position of forearm flexion and support with sling • Hand and finger • splint with tongue depressors, roller gauze and/or aluminum splints
Moving and Transporting Injured Athletes • Must be executed with techniques that will not result in additional injury • No excuse for poor handling • Planning is necessary and practice is essential • Additional equipment may be required
Proper Fit and Use of Crutches or Canes • When lower extremity ambulation is contraindicated • Faulty mechanics or improper fitting can result in additional injury or falls • Fitting athlete • Athlete should stand with good posture, in flat soled shoes • Crutches should be placed • 6” from outer margin of shoe • 2” in front of shoe • Crutch base should fall 1” below anterior fold of axilla (2 - 3 fingers) • Hand brace should be positioned to place elbow at 30 degrees of flexion • Cane measurement should be taken from height of greater trochanter
Walking with Cane or Crutch • Corresponds to walking • Tripod method • Swing through without injured limb making contact with ground • Four- point crutch gait • Foot and crutch on same side move forward simultaneously with weight bearing
Cane Tripod technique • Used on level surface • Modified with stair climbing • Unaffected support leg moves up one step (good goes up first) • Body weight is supported on crutch • Affected leg is pulled up to step • Reversed when descending stairs • Unaffected or good leg is used to lower • Affected leg and crutch (bad goes first) • Crutch walking follows a progression • Non-weight bearing (NWB) • Touch down weight bearing(TDWB) • Partial (PWB) • Full weight bearing (FWB) • When using cane or one crutch, support should be held on affected side