Download
1 / 30
300 likes | 465 Views
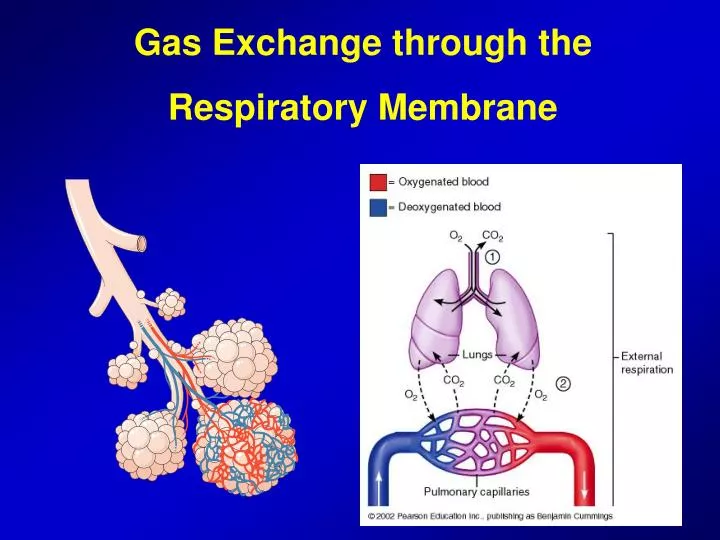
Gas Exchange through the Respiratory Membrane. Physics of gas diffusion. Molecular basis of gas diffusion Net diffusion of a gas in one direction: effect of a concentration gradient. Partial gas pressure. Gas pressures in a mixture of gases (Partial pressures of individual gases:

E N D
Physics of gas diffusion • Molecular basis of gas diffusion • Net diffusion of a gas in one direction: effect of a concentration gradient
Partial gas pressure • Gas pressures in a mixture of gases (Partial pressures of individual gases: • Respiratory physiology and O2, nitrogen and CO2 • Air composition: 79 % nitrogen and 21 % O2 • Total pressure of air at the sea level: 760 mmHg • Nitrogen: 600 mmHg and Oxygen: 160 mmHg • So partial pressure of O2 (Po2) is about 160 mmHg • Pressures of gases dissolved in water and tissues
Factors that determine partial pressure • The partial pressure of a gas is determined not only by its concentration but also by solubility coefficient of the gas • Henry’s law: • Partial p. = Conc.of dissolved gas/ Solubility coefficient • Net diffusion is determined by the difference between two partial pressures
Vapor Pressure of Water • When nonhumidified air is breathed into the respiratory passageways, water immediately evaporates from the surfaces of these passages.. • Water molecules escape from the water surface into the gas phase • Partial pressure that water molecules exert is called vapor pressure of the water • It is 47 mmHg at normal body temperature • PH2O is 47 mmHg • Importance of temperature
Quantifying the net rate of diffusion in fluids • In addition to pressure difference, several other factors affect the rate of gas diffusion in fluid • 1) Solubility of the gas in fluid • 2) Cross-sectional area of the fluid • 3) The distance through which gas must diffuse • 4) Molecular weight of the gas • 5) Temperature of the fluid • Respiratory gases are highly lipid soluble • So, major limitation to the movement of gases in tissues is the rate at which the gases can diffuse through the tissue water
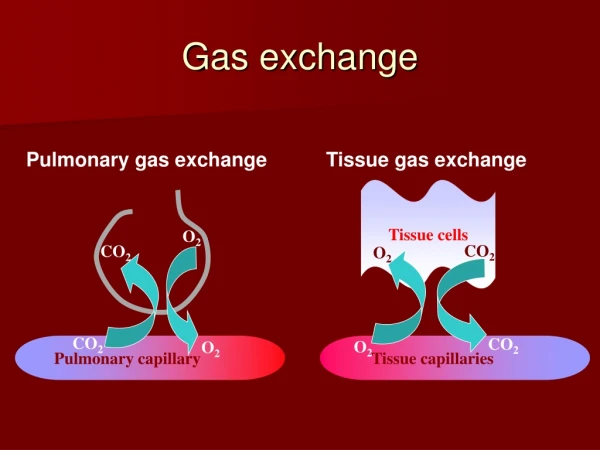
Composition of Alveolar Air vs Atmospheric Air • Alveolar air is only partially replaced by atmospheric air with each breath • Oxygen is constantly being absorbed into the pulmonary blood from the alveolar air • CO2 is constantly diffusing from the pulmonary blood into the alveoli • Dry atmospheric air is humidified before it reaches alveoli
Rate at which Alveolar Air is Renewed by Atmospheric Air • Functional residual capacity of the lungs (2300 ml) • Tidal volume and 350 ml of new air into the alveoli • Importance of slow replacement of alveolar air: prevention of sudden changes in tissue oxygenation, pH, CO2 level when respiration is temporarily interrupted
O2 Concentration and Partial Pressure in the Alveoli • The more oxygen is absorbed, the lower its concentration in the alveoli becomes or vice versa • 1) rate of absorption of O2 into the blood • 2) rate of entry of new O2 into the lungs by ventilation
O2 Concentration and Partial Pressure in the Alveoli • At normal ventilatory rate, O2 consumption is 250 ml/min • Moderate exercise and absorption of more O2 and maintenance of alveolar PO2 at normal rate of 104 mmHg • Alveolar ventilation can never increase the alveolar PO2 above 149 mmHg as long as breathing atmosph. air
CO2 Concentration and Partial Pressure in Alveoli • CO2 is continually being formed in the tissues and carried to the alveoli by blood • Normal rate of CO2 excretion: 200 ml/min • Normal alveolar PCO2 is 40 mmHg
Expired Air • Expired air is a combination of dead space air and alveolar air; its composition is determined by • Amount of expired air that is in dead space air • The amount that is alveolar air • Method of collecting alveolar air (last portion of expired air)
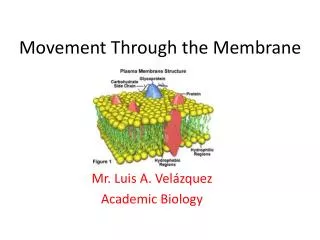
Respiratory Membrane • Respiratory unit: • Respiratory bronchiole, alveolar ducts, atria and alveoli • There are about 300 million alveoli in the two lungs • Alveoli are very thin (0.2 mm in diameter) and close to each other • All these membranes are called respiratory or pulmonary membrane
Surface Area and Thickness of the Respiratory Membrane • Respiratory membranes: • Are only 0.5 to 1 m thick, allowing for efficient gas exchange • Have a total surface area (in males) of about 60 m2 (40 times that of one’s skin) • Thicken if lungs become waterlogged and edematous, whereby gas exchange is inadequate and oxygen deprivation results • Decrease in surface area with emphysema, when walls of adjacent alveoli break through
Different layers of the respiratory membrane • Despite the number of layers, the thickness of respiratory membrane in some areas is 0.2 mm (average is 0.6 mm) • Total surface area of the respiratory membrane • Size of pulmonary capillaries (5 mm) and erythrocytes
Factors that affect the rate of gas diffusion through the respiratory membrane • The factors that determine how rapidly a gas will pass through the membrane: • 1) Thickness of the membrane • Edema, fibrosis… • 2) Surface area of the membrane • Emphysema • 3) Diffusion co-efficient of the gas in the membrane • 4) Partial pressure difference of the gas between the two sides of the membrane
Diffusion capacity of the respiratory membrane • The ability of the respiratory membrane to exchange a gas between the alveoli and pulmonary blood is expressed in quantitative terms (diffusing capacity) • Diffusing capacity for O2 at rest is 21 ml/min/mmHg • Mean O2 difference is 11 mmHg • So 11 x 21 = 230 ml O2 per min • Change in O2 diffusing capacity during exercise • Opennin up of many previously dormant pulmonary capillaries • A better match between ventilation and perfusion areas
Effect of Ventilation Perfusion Ratio on Alveolar Gas Concentration • Two factors determine the PO2 and PCO2 in the alveoli • Rate of alveolar ventilation • Rate of transfer of O2 and CO2 through respiratory membrane • Ventilation-perfusion ratio (VA/Q) some areas are ventilated but have no blood flow, other areas may have excellent blood flow but little or no ventilation • Alveolar O2 and CO2 partial pressure when VA/Q = 0 • There is no ventilation, and alveolar air comes to an equlibrium with blood O2 and CO2 • Venous blood has PO2 of 40 mmHg and PCO2 of 45 mmHg • These will be the normal partial pressures in the alveoli when VA/Q=0
Effect of Ventilation Perfusion Ratio on Alveolar Gas Concentration • Alveolar O2 and CO2 partial pressure when VA/Q = ∞ • There is no capillary blood flow • Instead of alveolar air coming to an equlibrium with the venous blood, it becomes equal to the humidified inspired air (PO2 = 149 mmHg) • Alveolar O2 and CO2 partial pressure when VA/Q is normal • PO2 in the alveolar air is normally 104 mmHg • PCO2 in the alveolar air is normally 40 mmHg
Concept of Physiologic Shunt • In this case, VA/Q ratio is below normal • Shunted blood • Blood fraction that flows through unventilated areas • The bronchial blood that is about 2% of cardiac output is also unoxygenated blood • Total quantitative amount of shunted blood per min is called physiologic shunt • The greater the physiologic shunt, the greater the amount of blood that fails to be oxygenated as it passes through the lungs
Concept of Physiologic Dead Space • In this case, VA/Q ratio is greater than normal • Ventilation is normal but capillary blood flow is low • There is far more O2 in the alveoli than can be transported away from the alveoli by the flowing blood • Thus, ventilation of these alveoli is “wasted” • Physiologic dead space can be calculated by using Bohr equation:
Abnormalities of Ventilation – Perfusion Ratio • Abnormal VA/Q in the uppper and lower normal lung • VA/Q is as much as 2.5 times as great as the ideal value • At the bottom of the lung, there is slightly too little ventilation in relation to blood flow with VA/Q as low as 0.6 times the ideal value • Abnormal VA/Q in chronic obstructive lung disease: • In COPD, some areas of the lung exhibit serious physiologic shunt and other areas exhibit serious physiologic dead space • Emphysema and smoking