Download
1 / 38
390 likes | 634 Views
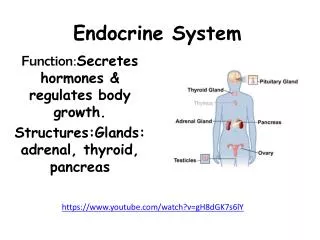
Endocrine Emergency. Chatlert Pongchaiyakul MD. - Hypoglycemia - Diabetic ketoacidosis - Hyperosmolar non - ketotic coma - Focal hyperglycemic seizure. - Thyroid Crisis - Myxedema Coma - Adrenal crisis - Hypercalcemia - Acute hypocalcemia. Hypoglycemia.

E N D
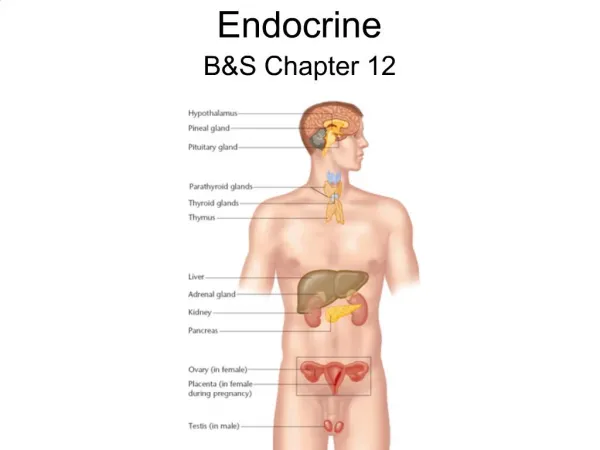
Endocrine Emergency Chatlert Pongchaiyakul MD.
- Hypoglycemia - Diabetic ketoacidosis - Hyperosmolar non - ketotic coma - Focal hyperglycemic seizure
- Thyroid Crisis - Myxedema Coma - Adrenal crisis - Hypercalcemia - Acute hypocalcemia
Hypoglycemia ระดับ Plasma glucose ต่ำกว่า 50 mg/dl “Whipple’s triad” - low plasma glucose - Neuroglycopenia - Corrected by glucose
Classification • Fasting hypoglycemia - underproduction - overutilization • Post prandial hypoglycemia
Underproduction of glucose • Hormone deficiency • Enzyme defect • Substrate deficiency • Acquired liver disease • Drug : alcohol, propanolol, salicylate,quinine etc.
Overutilization of glucose Hyperinsulinism • Insulinoma • Exogenous insulin • Sulfonylurea Appropriate insulin • Extrapancreatic tumor • Carnitine deficiency
Treatment • Good conscious • Oral intake • Correct cause of hypoglycemia • Monitor plasma glucose
Unconscious • 50% glucose 50 ml IV. ตามด้วย 10% Dextrose intravenous drip 125 - 250 ml/hr. • Glucagon 1 mg IM
Diabetic Emergency • DKA • HONC • Focal hyperglycemia seizure
DKA • Kussmaul’s breathing • Polyuria, polydipsia, polyphagia • Alteration of conscious • Other : dehydration, nausea, abdominal pain etc.
Diagnosis • Plasma glucose > 300-350 mg/dl • Wide anion gap acidosis • Serum Ketone + ve • not necessary
HONC • Neurological Sign & Symptoms • Severe Dehydration • Evidence of infection
Diagnosis - Plasma glucose > 600 mg/dl - Effective Osmolarity > 320 mOsm/lit - Serum Osmolarity > 340 mOsm/lit - PH > 7.30 - HCO3 > 15 mEq/lit - Prerenal azotemia
Treatment • Initial lab CBC, UA, BS, BUN, Cr, Electrolyte, ketone, ABG. Calculated osmolarity Septic work up
Fluid 0.9% Na Cl 1000 - 1500 CC. ในชั่วโมงแรก1000 CC.ในชั่วโมงที่ 2500 CC.ในชั่วโมงที่ 3 250 CC.ในชั่วโมงที่ 4 และต่อไป- ถ้า Na > 150 0.45% Na Cl- ผู้ป่วยสูงอายุ CVP
Insulin • Short actig (IV / IM) - 10 u IV. - 10 u IV drip / hr. (ผสมใน Na Cl) • Monitor BS q 1 hr. Electrolyte q 2-4 hr, osmolarity, Anion gap
BS < 300 เปลี่ยน 5%DW หรือ 5% DN/2 125-250 ml/hr. Insulin 10-12 u Sc. q 4 hr. หรือ IV.drip low dose (2 u/hr) NaHCO3 - pH < 6.9, 7.0 - Cardiovascular instability : 100 mEq IV drip in 1 hr.
Potassium If serum K 3 mEq ให้ KCl 30 mEq/hr. serum K 3-4 mEq ให้ KCl 20 mEq/hr. serum K 4-5 mEq ให้ KCl 15 mEq/hr. serum K 5-6 mEq ให้ KCl 10 mEq/hr. serum K 6 mEq ไม่ให้ KCl idividual adjustment with monitoring
THYROID STORM • Underlying hyperthyroidism • Without treatment, inadequate treatment • Precipitating cause
Precipitating Cause 1. Inappropriate treatment 2. Surgery 3. Infection 4. Injury 5. Radioactive iodine
Principle 1. Supportive treatment 2. Specific treatment 3. Correct prcipitating Cause
Specific treatment • Inhibit thyroid hormone synthesis • Inhibit thyroid hormone secretion • Inhibit thyroid hormone at peripheral tissue
PTU • Inh. Synthesis, secretion, periphecal conversion (T4 T3) • 900 - 1200 mg/d x 1-2 d. (4 x 4, 4 x 6, 2x12) • ฏ dose 600 mg/dl • 3 x 3 (450 mg/d) x 3 wk Definite treatment
Iodine • Lugol’s solution (10 mg/drop) 10 drops q 8 hr. • SSKI (50 mg/drop) 4 drops q 8 hr.
Correct precipitating cause • Infection • Surgery • Advice antithyroid drug
Controversy • - blocker : 40 mg q 4 - 6 hr. - oral (propanolol) 1 mg/min IV drip Corticosteroid : Dexamethasone 2 mg IV q 6 hr.
Practical point 1. ในกรณีไม่แน่ใจว่า Thyroid storm หรือ severe hyperthyroidism ให้รักษาแบบ thyroid strom ไว้ก่อน 2. การให้ propanolol ยัง Controversy 3. ถ้าจะให้ corticosteroid ต้องแน่ใจว่า สามารถควบคุมการติดเชื้อได้ดี
4. ถ้าเกิด thyroid strom หลังผ่าตัดให้ พิจารณา PTU / MMI rectal suppository, contrast media injection 5. ต้องให้ Lugol’s solution หรือ SSKI หลังจากให้ PTU ไปแล้ว 1 ชั่วโมง 6. ไม่ต้องรอผล thyroid function test
Myxedema Coma • Hypothyroidisim • Thyroidectomy scar • History of I 131 treatment
Precipitating cause 1. Infection 2. Sedative drug 3. การได้รับน้ำเกลือที่เป็น hypotonicity 4. Cold temperature
Symptoms & signs • Sign of hypothyroidism • Hypothermia • Bradycardia • Hypoventilation • Hyponatremia • Coma
Investigation • Routine lab • TFT, Electrolyte • EKG - low voltage - Flattening or inverted T-Waves
Principle 1. Supportive treatment 2. Specific treatment 3. Correct precipitating Cause
Supportive treatment • Body temperature • Correct hypoventilation • Correct hyponatremia • Coma care • Hydrocortisone 300 mg IV in 24 hr.
Specific treatment • Eltroxin - 400 - 500 ug IV drip slow Day 1 or 1000 ug NG - tube - Onset 6 hr. - ฏ dose 100 ug/d ในวันถัดไป
Correct precipitating cause • Evidence of infection and treatment • Stop sedative drug • Advice Medication