Download
1 / 51
510 likes | 620 Views
Gastrointestinal System Biomedicine Review. Felix Hernandez, M.D. Anatomy/Physiology. Responsible for the intake, digestion of food, absorption of nutrients, and elimination of solid waste. Alimentary Canal (GI tract). Accessory Digestive Organs. Teeth tongue salivary glands liver

E N D
Gastrointestinal System Biomedicine Review • Felix Hernandez, M.D.
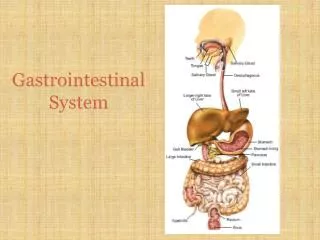
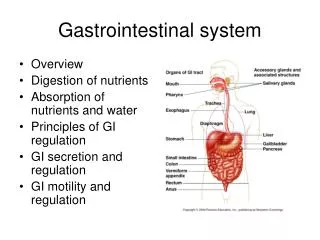
Anatomy/Physiology • Responsible for the intake, digestion of food, absorption of nutrients, and elimination of solid waste. • Alimentary Canal (GI tract)
Accessory Digestive Organs • Teeth • tongue • salivary glands • liver • gallbladder • pancreas
Teeth • Maxillary arch (upper) • Mandibular arch (lower) • anterior teeth for biting and tearing • posterior teeth for chewing and grinding
Oral Cavity • Palate, hard and soft • bolus • Pharynx • Uvula • Esophagus • Epiglottis
Esophagus • chyme • cardiac, or lower esophageal or gastroesophageal sphincter
Stomach • Body, fundus • pylorus • rugae • pyloric sphincter Fundus Body
Small Intestine • small bowel • villi • Parts • duodenum • jejunum • ileum • ileocecal valve
Large Intestine • Large Bowel • colon • cecum • vermiform appendix
Large Intestine • Colon • ascending • hepatic flexure • transverse • splenic flexure • descending • Sigmoid • Rectum • Anus
Liver • Functions • production of bile • glucose - glycogen • storage of vitamins, B12, A, D, E, K • erythrocytolysis (pigment released eliminated in bile called bilirubin) • bilirubin gives stool its characteristic dark color • removes toxins from blood • manufactures blood proteins
Pancreas • internal - endocrine function • insulin • glucogon • external - exocrine function • amylase - carbohydrates • trypsin, chymotrypsin - proteins • lipase - fats • enzymes inactive until reach duodenum
Gallbladder • pear-shaped sac under the liver • chol/e means bile or gall • cyst/o means cyst or sac • gallbladder contracts forcing bile out cystic duct into common bile duct.
Bile • bile is a digestive juice- emulsifier acts on fat in a way that lipid enzymes can digest fat • travels via hepatic duct to cystic duct to gall bladder, where stored • bile consists of water, bile salts, cholesterol, and bilirubin (a colored substance resulting from breakdown of hemoglobin) • bilirubin gives bile yellow or orange color
Stomach during Digestion • Gastric juices • HCL - activates enzymes • protease • pepsin • lipase • Chyme
Small Intestine during Digestion • digestion completed in small intestine • chyme mixed with bile and pancreatic juices • emulsification • absorption
Large Intestine • receive fluid waste products and store until released from body. • excess water absorbed • feces, stools • defecation, or bowel movement
Diseases of the Esophagus—Clinical Presentations • Dysphagia • Esophageal (retrosternal) pain • Aspiration or regurgitation
Diseases of the Esophagus • Developmental abnormalities—atresia with or without esophageal-tracheal fistula • Esophagitis • Hernia • Achalasia • Varices
Esophageal Atresia Figure 10-04A
Hiatal Hernia Figure 10-04B
Achalasia Figure 10-04C
Esophageal Varices Figure 10-04D
Esophagitis • Reflux of gastric juice (“peptic esophagitis”) • Infection—viruses, fungi (immunosuppressed persons), and bacterial superinfection • Chemical irritants—exogenous chemicals or drugs
Carcinoma of the Esophagus • Squamous cell carcinoma in upper or lower esophagus • Adenocarcinoma in lower esophagus developing in Barrett’s esophagus
Diseases of Stomach and Duodenum—Symptoms • Pain—midline, upper abdomen • Vomiting • Bleeding—acute with hematemesis or chronic with melena • Dyspepsia • Systemic consequences—e.g., iron deficiency anemia caused by chronic blood loss, vitamin B12 malabsorption–related megaloblastic anemia
Gastritis • Acute (erosive)—stress related, shock, food, exogenous chemicals and drugs • Erosions • Ulcerations • Chronic atrophic gastritis with or without intestinal metaplasia • Helicobacter pylori related • Autoimmune (with pernicious anemia)
Peptic Ulcer—Etiology and Pathogenesis • Multifactorial! • Contributing factors include: • Gastric juice—HCl, pepsin • Mucosal barrier defects—stress, shock, NSAIDs, smoking reduce resistance • Helicobacter pylori—found in most patients
Acid Reducing Agents • Histamine Receptor Blockers: • MOA: Histamine receptor Antagonist • Indications: duodenal/gastric ulcer, hypersecretion of acid, GERD • Interactions: increases concentration of anticoagulants • Drugs: • Cimetidine (Tagamet) • Ranitidine (Zantac) • Famotidine (Pepcid)
Proton Pump Inhibitors • Drugs: Omeprazole (Prilosec), Lansoprazole (Prevacid), Esomeprazole (Nexium), Pantoprazole (Protonix) • MOA: inhibits hydrogen/potassium ATPase (Proton pump) of the parietal cells thus reducing acid secretion. • Indications: reflux esophagitis, duodenal ulcers, hypersecretory states • Side Effects: Constipation (few side effects)
Mucosal Protectant • Misoprostol • MOA: increases bicarbonate and mucin release in the GI tract and reduces acid secretion • Indications: prevention of ulcers caused by aspirin and other NSAIDS • Side Effects: Abortion (uterine contraction) • Contraindications: PREGNANCY!!!! • Is a prostaglandin analog
Diverticulosis of the Colon Figure 10-08
Inflammatory Bowel Disease • Crohn’s disease—incidence is 70 to 150 per 100,000 persons per year in the United States • Ulcerative colitis—incidence is 20 to 40 per 100,000 persons per year in the United States • Cause unknown but may be familial
Inflammatory Bowel Agents • Mesalamine and Sulfasalazine • MOA: anti inflammatory • Indications: inflammatory bowel syndrome, UC or Crohn’s
Comparison of Diarrhea Caused by Small and Large Intestinal Disease
Antidiarrheal Agents • Opiates • Diphenoxylate and Atropine (Lomotil) • MOA: diphenoxylate is an agonist at opiate receptors in the GI tract and atropine blocks muscarinic receptors. Both of these actions inhibit peristalsis • Indications: Diarrhea • Side Effects: few such as constipation, abdominal/bowel distention • Contraindications: Parasitic or bacterial infections, obstructive jaundice • Increased risk of paralytic ileus with antimuscarinics • Loperamide (Imodium) • No drug interactions • Treat OD with Naloxone
Antidiarrheal Agents • Bismuth Subsalicylate (Pepto-Bismol) • MOA: absorbs toxins produced by bacteria and other GI irritants • Indications: Diarrhea, prophylaxis for traveler’s diarrhea • Side Effects: Impaction • Contraindications: Aspirin sensitivity • Kaolin/Pectin (Kaopectate) • MOA: adsorbent and protection that is of questionable efficacy • Indications: diarrhea
Acute Appendicitis Figure 10-12A
Acute Appendicitis Figure 10-12B
Acute Appendicitis Figure 10-12C
Intestinal Obstructions—Hernia Figure 10-13A
Intestinal Obstructions—Intussusception Figure 10-13B
Intestinal Obstructions—Volvulus Figure 10-13C
Malabsorption Resulting from Defective Uptake of Nutrients • Celiac sprue • Gluten • Tropical sprue • Infectious
Dysmotility Agent • Metoclopramide (Reglan) • MOA: increases rate of gastric emptying by an unknown mechanism • Indications: reflux esophagitis, gastroparesis, pre-op gastric emptying
Bulk Forming Agents • Psyllium (Metamucil) • MOA: nondigested plant cell wall absorbs water into feces thus softening the stool • Indications: constipation, hard stools • Side Effects: flatulence, impaction if the bolus is obstructed
Milk of Magnesia • Milk of Magnesia (saline solutions) • MOA: magnesium or sodium salts are poorly absorbed and thus draw water into the lumen. • High dose rids bowel of parasites and empties bowel preoperatively • Side Effects: precipitation of cardiac, renal, convulsive disorders or hypocalcaemia
Docusate (Colace) • MOA: improves penetration of water and fat into feces • Side Effects: diarrhea, abdominal cramps.