Download
1 / 37
370 likes | 531 Views
Putting it all together. JACQUE SCHOLL, AUD OKLAHOMA STATE UNIVERSITY - TULSA. Agenda. Why we need to do something different? Do our current practices predict success with amplification? Why do we need EBP and how would it help? Establishing an overall rehab plan .

E N D
Putting it all together JACQUE SCHOLL, AUD OKLAHOMA STATE UNIVERSITY - TULSA
Agenda • Why we need to do something different? • Do our current practices predict success with amplification? • Why do we need EBP and how would it help? • Establishing an overall rehab plan
Why we need to do something different? • Expectations • Unnecessary follow up visits • Less than desired satisfaction • RFC
Expectations vs. Goals • Expectations have a product orientation • Patient assumes passive role • Whatever goes wrong is the professional’s fault • Goals have a rehabilitation orientation • Patient assumes active role • Patient shares in the process
“Blessed is he who expects nothing, for he will not be disappointed” • Ambrose Bierce
Elements of Communication (Kiessling, et al,2003; Sweetow and Henderson-Sabes, 2004)
Goal is to relieve HANDICAPPING effects (WHO, 1997) • Audiogram doesn’t show these effects • This information is obtained through counseling • These effects are constantly changing
What constitutes a “typical” evaluation? • Pure tone audiogram • Middle ear assessment - sometimes • OAEs - sometimes • Monosyllabic speech testing in quiet • LDLs, MCLs, and RECDs – sometimes • Sentence recognition in noise - sometimes • Informational counseling
Based on research • There are three separate and distinct measures of hearing aid outcome • Usage • Subjective satisfaction and benefit • Speech intelligibility performance Humes (2003)
Speech intelligibility, satisfaction, and RFC • No evidence of relationship between unaided speech intelligibility scores and self-reports of satisfaction and benefit • No evidence of correlation between RFC and unaided speech Taylor, 2007
Current speech perception tests…. • Don’t take the contextual nature of conversation into account • Don’t take the interactive nature of conversation into account • Don’t allow access to conversational repair strategies that occur in real life Flynn, 2003
Hearing aid patients by age % Age (years) From Strom, Hearing Review, 2001
Perceptual and cognitive declines (resource limitations) in elderly • Speed of processing • Working memory • Attention difficulties (noise, distraction and executive control) Wingfield and Tun, 2001- Seminars in Hearing
Working Memory • Short-term memory: depicted in terms of storage capacity. • Working memory: capacity-limited, stores recent info, provides computational mental workspace to manipulate and integrate with long-term memory. • Limited capacity that is shared between processing and storage • Limits exceeded if processing too effortful or if more time is needed. Pichora-Fuller 2003
Impact of aging on speech perception • Even in the absence of hearing loss, older subjects require 3-5 dB higher SNR than young listeners (Schneider, Daneman and Murphy, 2005). • Older subjects with normal hearing perform approximately the same as young hearing impaired subjects (Wingfield and Tun, 2001)
Pichora-Fuller, 2006 Perhaps the problem isn’t that older people have true cognitive differences than young. Rather, the need for greater SNR places a greater strain on the cognitive resources. This creates more effortful listening.
Potential impediments to achieving mastery of these elements • Hearing loss • “Although it is true that mere detection of a sound does not ensure its recognition, it is even more true that without detection the probability of correct identification is greatly diminished”. (Pascoe, 1980) • Global cognitive decline • Maladaptive compensatory behaviors • Neural plasticity and progressive neurodegeneration • Morest, 2004 • Loss of confidence • Saunders and Cienkowski (2002)
The biggest mistake we currently make may be… • Making hearing aids the focus of our attention, when the focus should be… • Enhancing communication
How to do it? • All patients should be told at the outset of the appointment (even during the scheduling) that they will be receiving: • a CNA (Communication Needs Assessment) and • an overall (ICEP) Individualized Communication Enhancement Plan that will consist of… • education and counseling • communication strategies • individualized auditory training • hearing aids and / or ALDs • group therapy
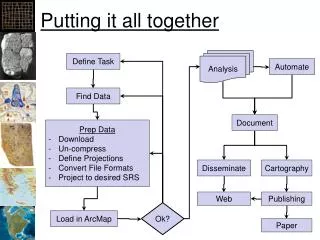
History Basic audiologic evaluation Communication Needs Assessment (CNA) Results Individual Communication Enhancement Plan (ICEP)
Relevant Domains for CNA • Communication expectations and needs • Sentence recognition in noise • Tolerance of noise • Ability to handle rapid speech • Binaural integration (interference) • Cognitive skills (working memory, speed of processing, executive function) • Auditory scene analysis • Perceived handicap • Confidence / self-efficacy
Communication Needs Assessment Measures beyond the audiogram that can be used to define residual auditory function. Objective procedures • QuickSIN • BKB-SIN • Hearing in Noise Test (HINT) • Words in Noise (WIN) • Acceptable Noise Levels (ANL) • Binaural interference • Dichotic testing • Listening span • TEN • Rapid (compressed) speech test • Speechreading • Dual-tasking
Communication Needs Assessment Measures beyond the audiogram that can be used to define residual auditory function. Subjective measures • Hearing Handicap Inventory for the Elderly – Screening HHIE-S • The Hearing Handicap Inventory for Adults (HHIA) • Communication Scale for Older Adults (CSOA) • Communication Confidence Test • Communication partner subjective scales (SAC and SOAC) Combined (objective and subjective) methods • Performance Perceptual Test (PPT)
The Individual Communication Enhancement Plan • may include any or all of the following: • A plan for learning about their particular hearing loss • A training program that may be completed at home or in the clinic • Hearing aids fitted to their specific hearing loss and communication needs and/or other hearing assistive devices, including alerting and listening devices, and subsequent detailed instruction and demonstration regarding the use and care of these devices • Workshops to learn more about living effectively with hearing loss • Counseling for the patients and members of their support system to enhance participation and address emotional and practical limitations • Return visit(s) to assess the effectiveness of the communication program. • Referral to other professionals i.e. memory and aging center and/or psychologist • Referral to social agencies for support
Aural (auditory, audiologic) rehab…… Should NOT be considered an add-on! Incorporate it at the very beginning
Training is not a new concept…. But now we have the means to do it effectively……via computer aided auditory rehabilitation….so that….. • It can be performed in a private, non-threatening environment • It can proceed at the individual’s optimal pace • Progress assessment can be done automatically
What do we do for a patient receiving an artificial limb? What do we do for a cochlear implant patient? What do we do for a patient with a balance disorder? What do we do for a hearing impaired patient?
Guidelines for the Audiologic Management of Adult Hearing Impairment, AAA, 2006Self-Perception of Communication Needs, Performance, and Selection of Goals for Treatment • 1. Each patient should receive formal self-assessment instrument(s)/inventory(s) prior to fitting to establish communication needs, function, and goals. • 2. Goals should be patient specific and composed of both cognitive and affective characteristics. • 3. Post-fitting administration of these instrument(s) is necessary to validate benefits/satisfaction from amplification.
Guidelines for the Audiologic Management of Adult Hearing Impairment, AAA, 2006 Non-Auditory Needs Assessment 1. be aware of the non-auditory factors that may impact successful prognosis. 2. query or screen for issues related to general health, manual dexterity (finger sensitivity), near vision, support systems, motivation, and prior experience with amplification. 3. use self-assessment scales to assess hearing aid readiness. 4. consider cognitive abilities and personality assessment 5. maintain a list of professionals trained to deal with the above mentioned issues to whom patients might be referred.
Guidelines for the Audiologic Management of Adult Hearing Impairment, AAA, 2006Hearing Aid Orientation The following device-related information should be provided to each patient, and ideally to at least one family member or caregiver, as part of the hearing aid fitting process: • Hearing aid features (multiple programs, telephone coil, directional microphone settings, direct audio input, and other special features) • Insertion/removal • Battery use (size, how to change, disposal, purchase options) • Care and cleaning • Comfort • Feedback • Telephone use • Warranty protection
Guidelines for the Audiologic Management of Adult Hearing Impairment, AAA, 2006Hearing Aid Orientation (cont.) The following information should be reviewed with each patient, and ideally at least one family member or caregiver, as part of the hearing aid fitting process: • Wearing schedule • Goals and expectations • Adjusting to amplification: family, social, school, and work settings • Environment issues: restaurants, groups, movies, television • Improved hearing and listening strategies • Speechreading • Monaural/binaural hearing aid use • Post-fitting care
Guidelines for the Audiologic Management of Adult Hearing Impairment, AAA, 2006Counseling and Follow-Up 1. Post-fitting counseling and follow-up should be (a) provided to new hearing aid users and (b) offered to experienced users who have not received these services or who may want a “refresher” course. 2. The patient’s primary communication partner(s) should be included. 3. Counseling and follow-up can be provided in a group or individual format. 4. Patients should be informed that the full benefits from amplification may not be immediately apparent.
Guidelines for the Audiologic Management of Adult Hearing Impairment, AAA, 2006Assessing Outcomes • Subjective • Objective
Are we properly instructing our patients to assess outcome? • Hearing soft sounds • Louder perception • Understanding speech in noise Listening effort • End of day fatigue • Strategies • Quality of life • Benefit or satisfaction • RFC