Download

1 / 20
200 likes | 400 Views
The Effects of Statin Copayments and Statin Adherence on Medical Care Utilization and Expenditures. Teresa B. Gibson 1 , Ph.D.; Tami L. Mark 1 Ph.D., MBA; Kirsten Axelsen 2 , MS; Onur Baser 1 , Ph.D.; Joan A. Mackell 2 , Ph.D.; Heidi King 2 , MS; Kimberly A. McGuigan 2 , Ph.D., MBA

E N D
The Effects of Statin Copayments and Statin Adherence on Medical Care Utilization and Expenditures Teresa B. Gibson1, Ph.D.; Tami L. Mark1 Ph.D., MBA; Kirsten Axelsen2, MS; Onur Baser1, Ph.D.; Joan A. Mackell2, Ph.D.; Heidi King2, MS; Kimberly A. McGuigan2, Ph.D., MBA 1 Thomson Medstat, Ann Arbor, MI 2 Pfizer, Inc., New York, NY American College of Cardiology, 55th Annual Scientific Session March 14, 2006
Presenter Disclosure Information “The Effects of Statin Copayments and Statin Adherence on Medical Care Utilization and Expenditures” Disclosure Information...The following relationships exist related to this presentation: • T.B. Gibson, Research Grants, Pfizer, Inc., Significant • T.L. Mark, Research Grants, Pfizer, Inc. Significant • K. Axelsen, Salary, Pfizer, Inc., Significant • O. Baser, Research Grants, Pfizer, Inc., Significant • J.A. Mackell, Salary, Pfizer, Inc., Significant • H. King, Salary, Pfizer, Inc., Significant • K.A. McGuigan, Salary, Pfizer, Inc., Significant
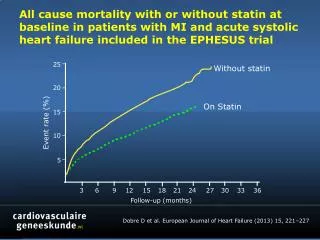
Introduction • HMG-CoA reductase inhibitor (“statin”) therapy is a widely accepted treatment for patients with high cholesterol. • Clinical trials report benefits such as reductions in mortality and morbidity from statin therapy (National Cholesterol Education Program(NCEP) Expert Panel 2002, and Simes et al. 2002). • The extent of cardiovascular risk reduction can increase in proportion to the amount of time on statin therapy (Simes et al. 2002)
Introduction (continued) • Prescription drug copayments have increased as employers and other plan managers attempt to contain prescription drug costs. (Kaiser Family Foundation and the Health Research and Educational Trust 2005) • Cost-sharing is likely to continue to rise. Many firms intend to continue to increase cost-sharing in the near future. (Kaiser Family Foundation and the Health Research and Educational Trust 2005; PriceWaterhouseCoopers 2005) • Higher prescription drug copayments may lead patients with chronic conditions to reduce utilization of maintenance drugs (Bierman and Bell 2004; Gibson et al. 2005) • Higher statin copayments are associated with a reduction in compliance for new users of statins. Higher statin copayments and lower levels of statin compliance are also related to lower levels of outcomes (e.g., LDL-C goal attainment and hospitalization). (Goldman et al. 2005, Schultz et al. 2005)
Study Aims • To estimate the effects of statin copayments on statin adherence for continuing users of statins, and, • To estimate the effects of statin adherence on expenditures and utilization
Data Source • MarketScan Commercial Claims and Encounter Database and Medicare Supplemental and Coordination of Benefits Database for services provided from January 1, 2000 through December 31, 2003. • Contains the healthcare experience of individuals with employer-sponsored health care insurance and Medicare supplemental insurance in the United States • Includes enrollment information and inpatient, outpatient and pharmacy claims
Inclusion Criteria and Study Sample • Inclusion Criteria: • 18 years of age or older • Continuously-enrolled from 2000 through 2003 • At least one statin prescription fill January 2001 through June 2001 • No indication of pregnancy during the study time frame • Study Sample Construction: • Continuing users: Filled a statin prescription in 2000 • Each patient was followed July 2001 through December 2003 • n=93,296 patients
Measures • Adherence to Statin Therapy (July 2001 – December 2002) • Medication Possession Ratio (MPR) calculated by assessing whether statins were on-hand each day, % of days with statins on-hand • Adherent if MPR > 80% • Expenditures and Utilization (January - December 2003) • Expenditures – • Total (Medical plus prescription drug) • Medical • Prescription Drug • Utilization (1/0 variables) • Physician Office Visit • Emergency Room Visit • Hospitalization • Coronary Heart Disease-related (CHD) Hospitalization
Explanatory Variables • Patient Cost-Sharing • Statin cost sharing amount ($ 2003 per day) • Office Visit cost sharing amount ($ 2003 per visit) • Sociodemographic - Age, Gender, US Census Region, Urban Area, Household Income and % with College Degree (by ZIP code via Census information) • Health Plan Type – (e.g., HMO, PPO, POS, Comprehensive) • Type of Provider (prior 12 months) • Medication (prior 12 months) - Number of prescriptions, Any use of mail order • Severity/Comorbidity (prior 12 months) • Acute Myocardial Infarction, Angioplasty, Coronary Bypass Surgery, Chronic Ischemic Heart Disease (IHD), Coronary Atherosclerosis, Other IHD, Hypertension • Anxiety, Dementia, Depression
Multivariate Analysis Part 1: Adherence, Logistic Regression • Pr(Adherencei|x) = F(0 + 1sociodemographici + 2plani + 3providerip + 4medicationip + 5severityip + 6comorbidityip + 7cost-sharingi) Part 2: Utilization and Expenditures • G(Expenditurei) = ln(0 + 1sociodemographici + 2plani + 3providerip + 4severityip + 5comorbidityip + 6E(Adherence)) • P(Utilizationi|x) = F(0 + 1sociodemographici + 2plani + 3providerip + 4severityip + 5comorbidityip + 6E(Adherence)) i is patient, p is a 12 month lag, F is the cumulative logistic function and G is the gamma distribution
Effects of Copayments on Adherence Predicted Probability of Adherence All p<.01 Higher copayments are associated with lower levels of adherence
Effects of Estimated Adherence on Expenditures Higher levels of adherence are associated with lower medical expenditures, higher prescription drug expenditures and no change in total expenditures
Effects of Estimated Adherence on Expenditures Estimated 2003 Expenditures * p<.10, *** p<.01
Effects of Estimated Adherence on Utilization Higher levels of adherence are associated with an increased likelihood of an office visit, and a decreased likelihood of ER visits, hospitalizations and CHD-related hospitalizations * p<.10,** p<.05, *** p<.01
Effects of Estimated Adherence on Utilization * p<.10,** p<.05, *** p<.01
Limitations • Administrative Data • Continuously-enrolled population with employer-sponsored insurance • Selection • Sensitivity Analysis
Summary and Conclusions • In this large cohort of continuing users of statins enrolled in employer-sponsored plans, prescription drug copayments are a financial barrier to statin adherence. • Reducing patient cost-sharing for a maintenance drug regime may be an effective intervention. • In turn, statin adherence is related to higher prescription drug expenditures and an offset in medical expenditures, but total expenditures are not significantly different. • Lower statin copayments are associated with higher levels of statin adherence. Total costs may not change, but fewer negative events (ER visits, hospitalizations and CHD-related hospitalizations) occur.